Translate this page into:
Scleromyxedema
Correspondence Address:
Jian-Fang Sun
Jiangwangmiao Street No. 12, Nanjing, Jiangsu, 210042
China
Wei Zhang
Jiangwangmiao Street No. 12, Nanjing, Jiangsu, 210042
China
| How to cite this article: Yang Y, Chen H, Zhang W, Sun JF. Scleromyxedema. Indian J Dermatol Venereol Leprol 2016;82:738-739 |
A 63-year-old male presented with a history of numerous papules on the neck, trunk and limbs for 2 years, partly in a linear arrangement, and progressive induration and thickening of the skin on the forehead and hands for 1 year [Figure - 1]a,[Figure - 1]b,[Figure - 1]c. Biopsy of a papule on the left arm revealed Alcian blue-positive mucinous material between thick collagen bundles and proliferation of fibroblasts in the dermis. [Figure - 1]d. Immunofixation electrophoresis revealed IgG monoclonal gammopathy with λ light chains. Thyroid gland function was normal.
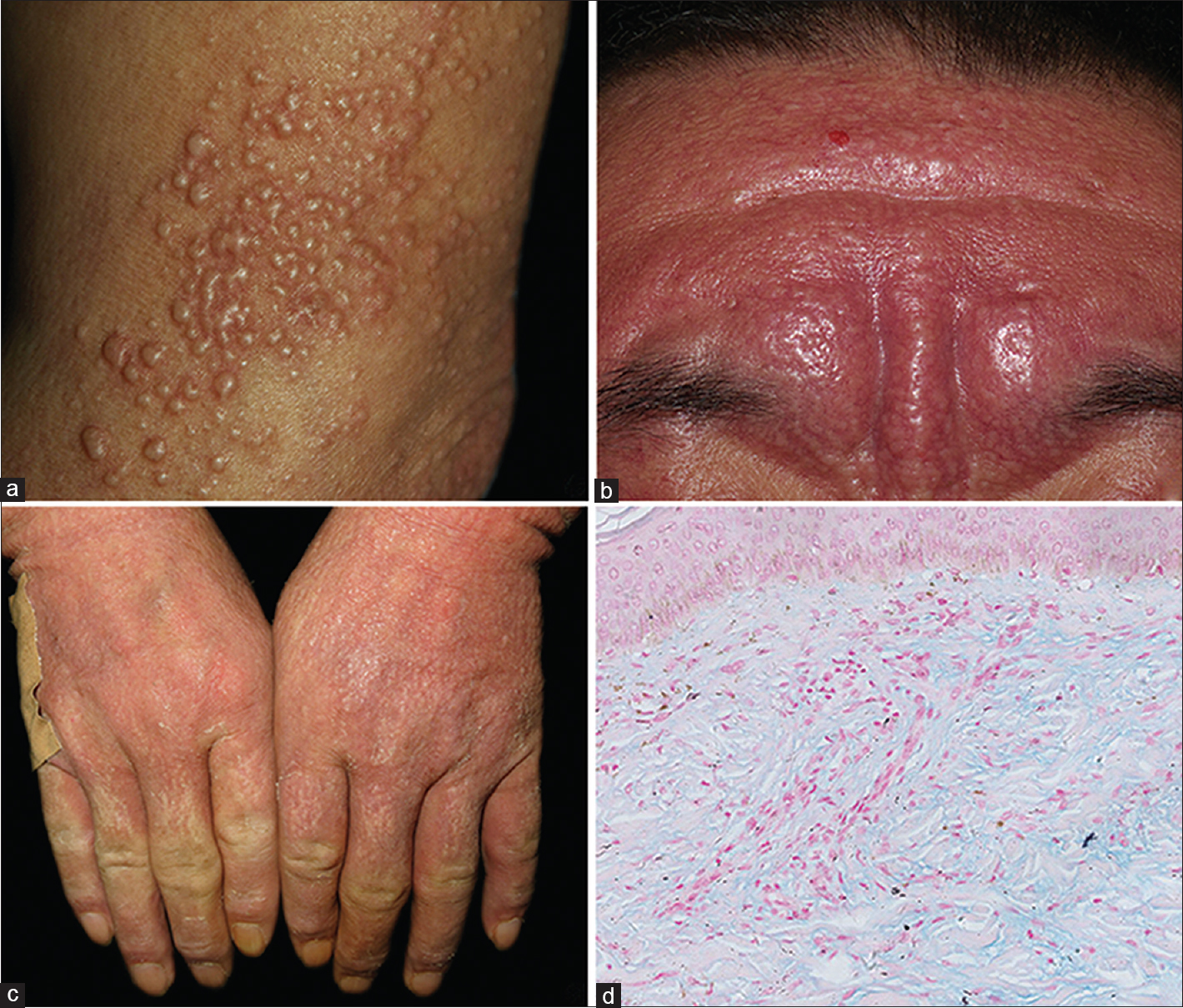 |
| Figure 1: Numerous firm papules and nodules distributed on the neck, trunk, and limbs (a), partly in a linear arrangement. Diffuse induration and thickening of the skin on the forehead (b) and hands (c). Positive alcian blue staining demonstrated mucin deposition (d) |
Scleromyxedema is a rare disease characterized by a generalized papular and sclerodermoid eruption, the histological triad of mucin deposition, fibroblast proliferation and fibrosis, monoclonal gammopathy, and absence of a thyroid disorder. Usually, treatment is unsatisfactory and systemic therapy may include melphalan, steroids, plasmapheresis, acitretin, immunoglobulin, thalidomide, methotrexate, cyclophosphamide, ciclosporin, and phototherapy. Recent reports recommended intravenous immunoglobulin (IVIG), which is relatively effective and safe but maintenance therapy is required to control disease.
Fulltext Views
8,034
PDF downloads
2,335





![[Figure - 1]](#fig_ijdvl_2016_82_6_738_174420_f1.jpg){kind=link}