Translate this page into:
Seborrheic keratosis coexisting with syringoma
Correspondence Address:
Gyong Moon Kim
Department of Dermatology, St. Vincent Hospital, College of Medicine, The Catholic University of Korea, 93 6, Ji dong, Paldal Ku, Suwon Si, 442 723
Korea
| How to cite this article: Lee JH, Won CY, Kim GM, Kim SY. Seborrheic keratosis coexisting with syringoma. Indian J Dermatol Venereol Leprol 2012;78:409 |
Sir,
Seborrheic keratosis (SK) is very common tumor on the trunk and face. It is unusual that SK coexists with other neoplasms. Basal cell carcinoma, Bowen′s disease, eccrine poroma and porocarcinoma have been reported in association with SK. [1] Syringoma is a benign neoplasm of sweat gland origin. The coexistence of syringoma with other types of tumors is rare. Syringoma has been reported in association with epidermal cyst, melanocytic nevus and basal cell carcinoma. [2] To our knowledge, coexistence of SK with syringoma has not been reported thus far.
A 48-year-old man presented with a 1.5-cm plaque on the scalp for 2 years. He noted that the lesion was slowly getting larger. He had diabetes mellitus. Physical examination revealed a verrucous and blackish plaque with a peripheral tan-brown ring [Figure - 1]. The clinical differential diagnosis was SK, verruca or basal cell carcinoma. A skin biopsy was performed. The upper part of the lesion showed markedly thickened epidermis composed of a proliferation of basaloid cells with pseudohorn cysts and basal melanosis [Figure - 2]a and b. On the other hand, the lower part of the same lesion revealed clusters of small ducts and strands composed of epithelial cells in a fibrous stroma [Figure - 2]c. This lesion was clearly distinguished from trichoepithelioma and sclerosing basal cell carcinoma. A final diagnosis was a typical SK accompanied with syringoma.
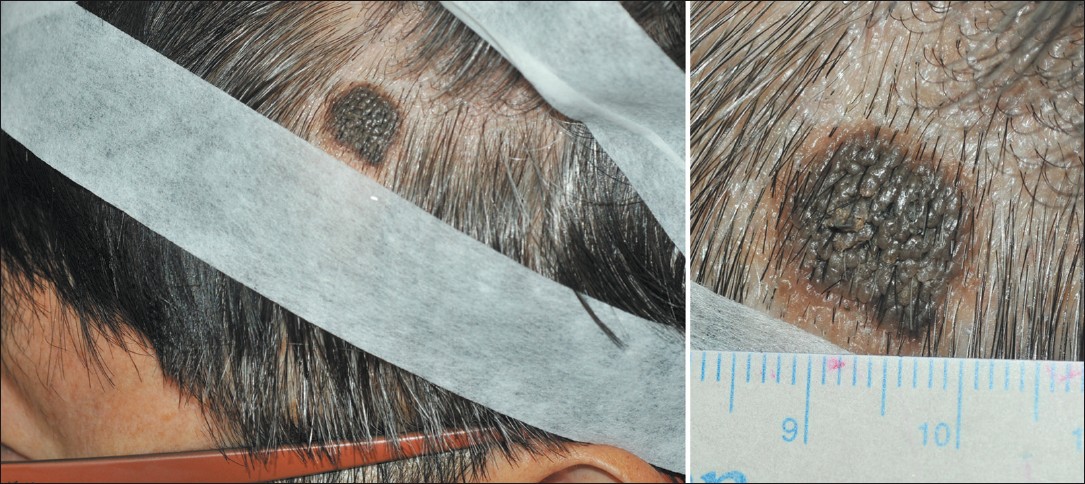 |
| Figure 1: A 1.5 cm - sized, verrucous, brownish plaque on the scalp |
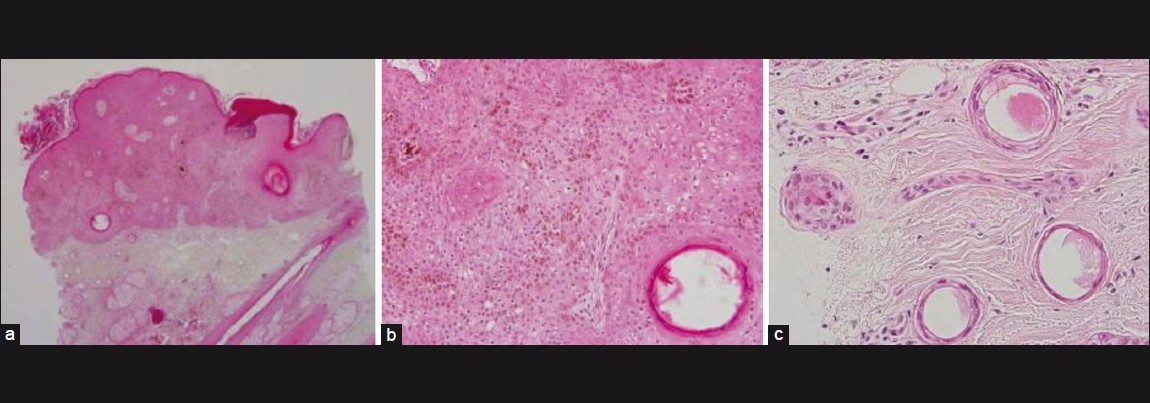 |
| Figure 2: (a) Biopsy specimen from the scalp showing thickened epidermis with interspersed horn cysts filled with keratin. Several tubular structures are embedded in a collagenous stroma [hematoxylin and eosin (H and E), ×100]. (b) In the epidermis, basaloid cells are small and uniform (H and E, ×200). (c) In the dermis, some ducts are lined by epithelial cells and some strands have comma-like tails of epithelial cells (H and E, ×400) |
Although SK is one of the most common skin lesions, the histogenesis of SK is not well elucidated. Monteagudo et al. suggested that SK is derived from the infundibular portion of the hair follicle. [3] This theory is supported by the fact that SK frequently occurs on hair-bearing skin. Some authors have suggested that SK is derived from the pluripotent epidermal basal cell that is vulnerable to local irritation, ultraviolet light and trauma. [4]
Syringoma is a common benign tumor that is composed of eccrine strands and ducts dispersed in a fibrous stroma, and usually occurs on the lower eyelid. Mehregan. suggested that ductal proliferation may be a reaction to an acute inflammatory process, fibrosis or the mechanical effect of the mass of a neoplasm associated with inflammatory disease, other neoplasms, hamartomas or cysts. [5] Namely, cystic dilatation seems to be a result of compression of the acrosyringium by proliferation of a mass such as basal cell carcinoma. [6] According to a recent report, syringoma is a tumor associated with intradermal mesenchymal change, and the stroma of syringoma lesions showed mast cells and some cytokines, such as IL-1α and IL-β. [6] It is still unknown whether SK could induce an eccrine tumor, whether this lesion is coincidental or whether there is a collision tumor.
In the case that we report here, syringoma might be induced by cytokines or mass effect from SK rather than by chance. Conversely, irritation triggered in a syringoma lesion may cause SK. We suggest that when SK does not respond to the standard treatment, clinically unapparent syringoma should be taken into consideration.
| 1. |
Madan V, Cox NH, Gangopadhayay M. Porocarcinoma arising in a broad clonal seborrhoeic keratosis. Clin Exp Dermatol 2008;33:350-1.
[Google Scholar]
|
| 2. |
De Sousa Fernandes B, Caviggioli F, Di Tommaso L. Basal cell carcinoma adjacent to syringoma in periorbital skin: A case report. Am J Dermatopathol 2005;27:362-3.
[Google Scholar]
|
| 3. |
Monteagudo JC, Jorda E, Terencio C, Llombart-Bosch A. Squamous cell carcinoma in situ (Bowen's disease) arising in seborrheic keratosis: Three lesions in two patients. J Cutan Pathol 1989;16:348-52.
[Google Scholar]
|
| 4. |
Rao BK, Freeman RG, Poulos EG, Arbesfeld L, Rendon M. The relationship between basal cell epithelioma and seborrheic keratosis. A study of 60 cases. J Dermatol Surg Oncol 1994;20:761-4.
[Google Scholar]
|
| 5. |
Mehregan AH. Proliferation of sweat ducts in certain diseases of the skin. Am J Dermatopathol 1981;3:27-31.
[Google Scholar]
|
| 6. |
Iwao F, Onozuka T, Kawashima T. Vulval syringoma successfully treated with tranilast. Br J Dermatol 2005;153:1228-30.
[Google Scholar]
|
Fulltext Views
3,338
PDF downloads
2,131





![[Figure - 1]](#fig_ijdvl_2012_78_3_409_95498_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_3_409_95498_f2.jpg){kind=link}