
Translate this page into:
Slow growing lesion on face

Corresponding author: Dr Shekhar Neema, Department of Dermatology, Base Hospital, Lucknow, India. shekharadvait@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Neema. S, Choudhary SR, Madakshira MG. Slow growing lesion on face. Indian J Dermatol Venereol Leprol. 2024;90:704. doi: 10.25259/IJDVL_1281_2023
A 65-year-old man, non-smoker and diabetic, presented with a single asymptomatic skin-coloured, raised lesion over his left cheek of two years duration. Dermatological examination revealed a firm, ill-defined, indurated nodular plaque with overlying telangiectatic vessels in the left infra-orbital region measuring approximately 7 cm × 4 cm in its largest diameter. [Figure 1]. No significant lymphadenopathy was appreciated. Systemic examination was within normal limits. Polarised dermoscopy showed a milky pink background, reticular pigment network, yellow structureless area, white structureless areas, chrysalis-like structures and linear irregular vessels and out-of-focus vessels [Figure 2]. Histopathological examination demonstrated variable-sized infiltrating islands of polygonal tumour cells with regular nuclei, small inconspicuous nucleoli and moderate dense eosinophilic cytoplasm [Figures 3a and 3b]. Immunochemistry (IHC) revealed tumour cells positivity for CK20 and synaptophysin while being negative for CK 7, HMB-45 and S100 [Figures 4a–4c].
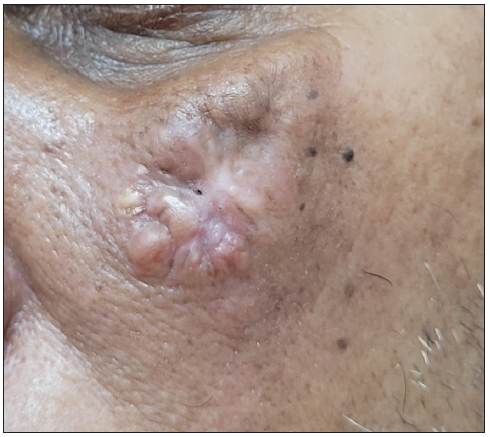
- Clinical image showing plaque over the left infraorbital region.
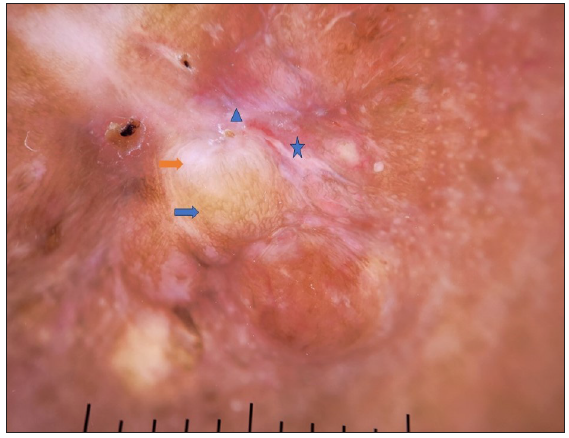
- Dermoscopy shows pink background, yellow structureless area (blue arrow), white structureless area (orange arrow), linear vessels (blue triangle) and chrysalis-like structure (blue star). (Dermlite DL4, polarised 10x).
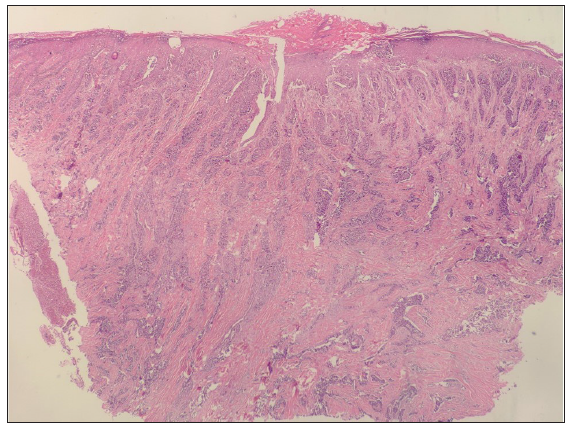
- Histopathology image shows epidermis with compact keratosis with flattened rete pigs. Dermis shows variable-sized infiltrating islands of monotonous tumour cells forming trabeculae (Haematoxylin and eosin, 40x).
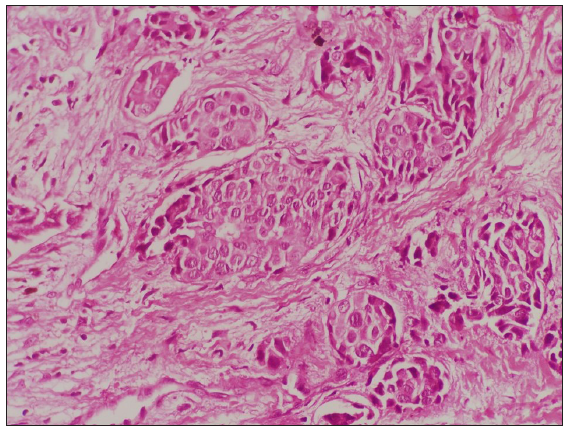
- Polygonal cells with regular nuclei and inconspicuous nucleoli (Haematoxylin and eosin, 1000x).
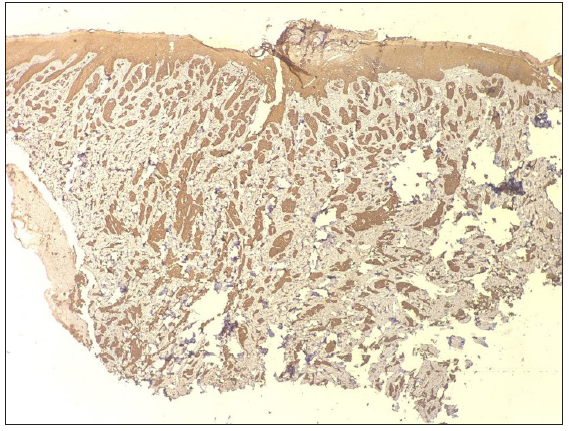
- Immunohistochemistry shows CK 20 positive (40x).
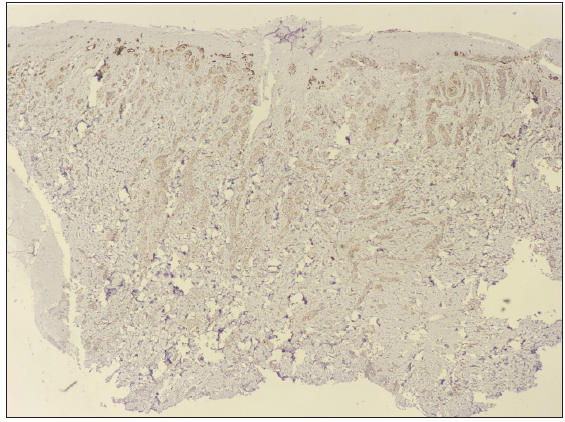
- Immunohistochemistry shows CK7 negative (40x).
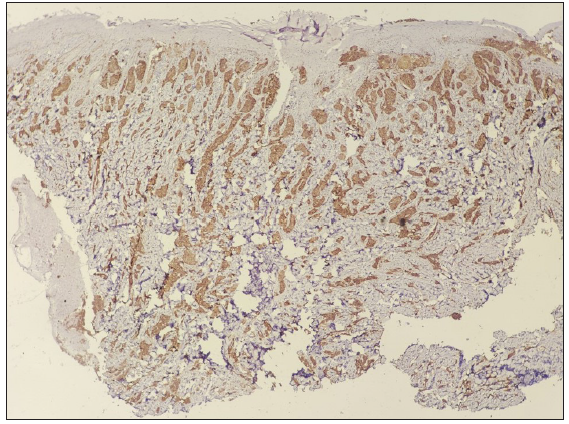
- Immunohistochemistry shows synaptophysin positive (40x).
Question
What is the diagnosis?
Answer
Merkel cell carcinoma.
Discussion
Merkel cell carcinoma (MCC; formerly called trabecular carcinoma) was first described by Toker in 1972.1 It typically presents as an asymptomatic, rapidly growing non-pigmented nodule in the elderly population, with a predilection for head and neck. In contrast, our patient’s tumour had gradually progressed over 2 years. Tumour cells of MCC originate from the epidermal progenitors, potentiated by the UV radiation’s mutagenic effects and morphologically mimic mechanoreceptor cells. It carries a poor prognosis with a mortality rate as high as 40%.2 In the year 2008, Feng et al. discovered the integration of the polyomavirus genome in the genome of MCC tumour cells, which was later designated as the Merkel cell carcinoma virus. Recently, compelling evidence of causation has led to its classification as a Group 2A carcinogen by the World Health Organisation (WHO) International Agency for Research on Cancer (IARC).2
In recent years, the global incidence has increased by 95%, possibly due to systemic immune-suppression, cumulative UV exposure and longer life span. Despite its aggressive nature, the diagnosis is delayed as it mimics various benign and malignant lesions. Spontaneous regression of the primary tumour has been observed in rare instances.1
The differential diagnosis with other cancers relies heavily on immunohistochemistry. Neuroendocrine markers such as neuron-specific enolase, synaptophysin, CD56 and chromogranin A, and epithelial proteins like cytokeratins, are positive. CK20 is a significant marker for MCC due to its specificity, however, it may not be expressed in 5% of patients.3
Treatment options for local disease include wide excision, adjuvant radiotherapy and sentinel-node biopsy. Being a highly aggressive neuroendocrine skin tumour with a propensity for early metastasis, early diagnosis is crucial for better outcomes.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Dermoscopy of merkel cell carcinoma. Dermatology. 2012;224:140-4.
- [CrossRef] [PubMed] [Google Scholar]
- Merkel cell polyomavirus is implicated in a subset of merkel cell carcinomas, in the indian subcontinent. Microb Pathog. 2019;137:103778.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Merkel cell carcinoma: Clinical, dermoscopic and immunohistochemical aspects of a rare tumor.
- [CrossRef] [Google Scholar]




