Translate this page into:
Slowly growing nodule in supralabial region
Correspondence Address:
Carlos Gonzalez-Cruz
Passeig de la Vall d'Hebron, 119-129, 08035 Barcelona
Spain
| How to cite this article: Gonzalez-Cruz C, Bodet D, Garcia-Patos V. Slowly growing nodule in supralabial region. Indian J Dermatol Venereol Leprol 2020;86:215-217 |
A 63-year-old man with a history of chronic obstructive pulmonary disease presented with a 16 mm × 15 mm solitary lobulated nodule in the right supralabial region. The tumor that appeared 15 years ago was slowly growing and asymptomatic. On physical examination, the tumor was firm, well-circumscribed, without pain on palpation and the overlying skin showed no inflammatory signs or abnormal pigmentation [Figure - 1]. An excisional biopsy was performed. The tumor was well delimited with no adhesions, which allowed complete removal. The histopathologic examination demonstrated a well-circumscribed dermal tumor [Figure - 2]a with clusters and solid cords of cells as well as ductal structures through a myxoid, chondroid and fibrous stroma. Keratinous cysts and calcifications were present [Figure - 2]b and [Figure - 2]c. Tubuloalveolar structures were lined internally by epithelial cells and externally by myoepithelial cells. Decapitation secretion was observed [Figure - 2]d. Surgical margins were not affected. No tumor recurrence occurred after 15 months of follow-up.
 |
| Figure 1: Firm and well-circumscribed solitary lobulated nodule in the right supralabial region |
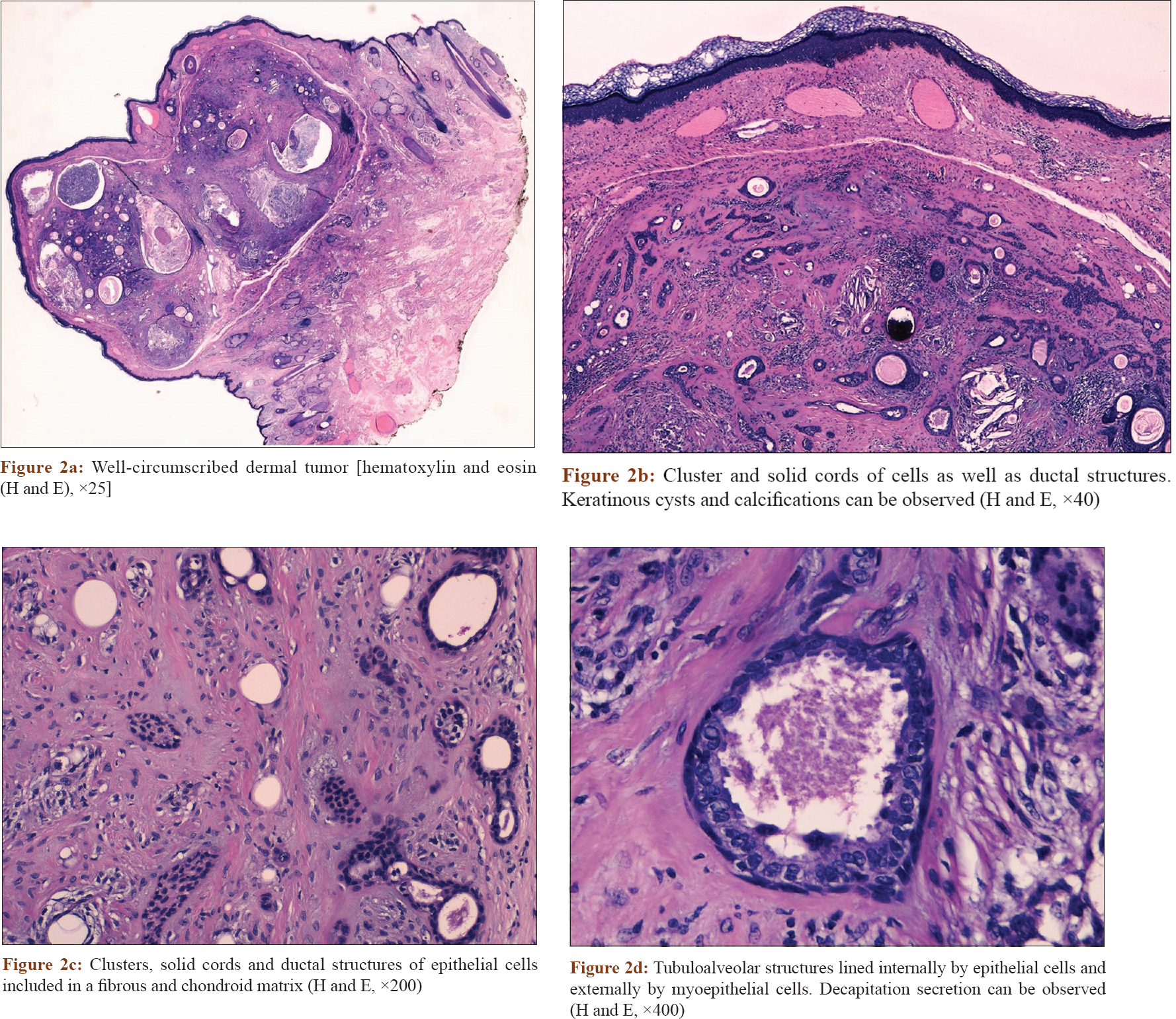 |
| Figure 2: |
Question
What is your diagnosis?
Acknowledgment
The authors thank Dr. Berta Ferrer for her help with the pathological images and Dr. Sabina Ruiz for revising the manuscript.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Villalón G, Monteagudo C, Martín JM, Ramón D, Alonso V, Jordá E, et al. Chondroid syringoma: A clinical and histological review of eight cases. Actas Dermosifiliogr 2006;97:573-7.
[Google Scholar]
|
| 2. |
Yavuzer R, Başterzi Y, Sari A, Bir F, Sezer C. Chondroid syringoma: A diagnosis more frequent than expected. Dermatol Surg 2003;29:179-81.
[Google Scholar]
|
| 3. |
Kazakov DV, Belousova IE, Bisceglia M, Calonje E, Emberger M, Grayson W, et al. Apocrine mixed tumor of the skin (“mixed tumor of the folliculosebaceous-apocrine complex”). Spectrum of differentiations and metaplastic changes in the epithelial, myoepithelial, and stromal components based on a histopathologic study of 244 cases. J Am Acad Dermatol 2007;57:467-83.
[Google Scholar]
|
| 4. |
Requena L, Sánchez Yus E, Santa Cruz DJ. Apocrine type of cutaneous mixed tumor with follicular and sebaceous differentiation. Am J Dermatopathol 1992;14:186-94.
[Google Scholar]
|
| 5. |
Odhav A, Odhav C, Odhav S. Diagnosis of a rapidly growing preauricular nodule: Chondroid syringoma or pleomorphic adenoma? Cutis 2016;98:E7-9.
[Google Scholar]
|
Fulltext Views
3,233
PDF downloads
4,955





![[Figure - 1]](#fig_ijdvl_2020_86_2_215_241411_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_2_215_241411_f2.jpg){kind=link}