Translate this page into:
Solitary painful red macule over left knee
2 Department of Pathology, All India Institute of Medical Sciences, New Delhi - 110029, India
Correspondence Address:
Binod K Khaitan
Department of Dermatology & Venereology, All India Institute of Medical Sciences, New Delhi - 110 029
India
| How to cite this article: Khaitan BK, Kaur J, Das AK. Solitary painful red macule over left knee. Indian J Dermatol Venereol Leprol 2006;72:327-328 |
 |
|
 |
|
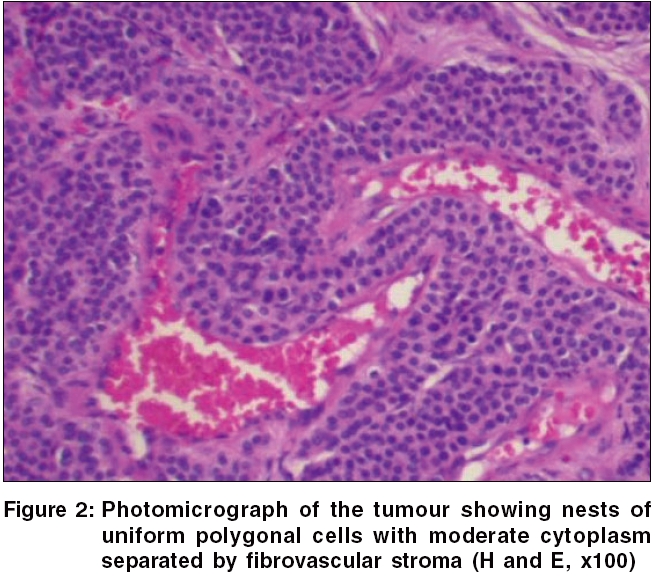
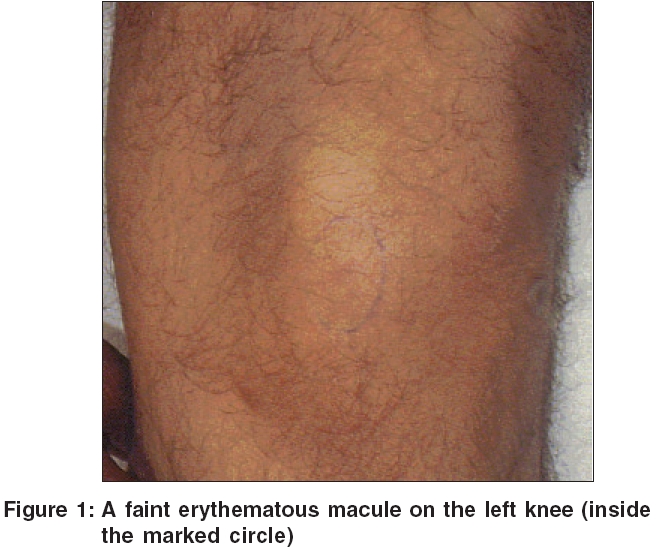
A 50-year-old man presented with a 3-year history of an ill-defined painful area on his left knee [Figure - 1]. The pain was transient lasting for a few seconds and used to precipitate by touch and even with light contact with clothing. There was no seasonal variation in the pain and it was not temperature- dependent. It had no correlation with the movements of the knee joint. On examination, there was a faint reddish macule of 3 mm-size on the lower part of left knee. A positive Love′s sign was observed with maximal tenderness, localized to a small pinhead area confined to the macule. The lesion was excised and histopathological examination showed normal epidermis and nests of round to polygonal cells in the dermis, having moderate amount of eosinophilic cytoplasm and round nuclei with prominent nucleoli in some. The cellular nests were separated by fibrocollagenous tissue containing numerous dilated blood vessels [Figure - 2]. In one year of follow-up, no recurrence was observed.
What is your diagnosis?
Diagnosis: Extradigital glomus tumor
Discussion
Glomus tumour, a benign growth arising from the glomus apparatus in the skin, occurs most frequently on fingers and toes. Its clinical diagnosis is easy on these usual sites, but it may pose a difficulty if it occurs on an extradigital location. Glomus tumours are relatively rare vascular tumours, with a reported incidence of 1.6% of all soft tissue tumours.[1] A solitary glomus tumour is a pink or purple nodule with a classic triad of pain, cold sensitivity and point tenderness.[2] The commonest site is the hands, particularly the fingers. Tumours beneath the nails are extremely painful and present early, with affected nail showing just a bluish red flush. The diagnosis of glomus tumour is readily suspected when it is present in classical subungual location, but lesions occurring elsewhere may pose a diagnostic difficulty. This has been noted in the literature, with reports of unusual locations of glomus tumour of ankle,[3] foot,[4] knee,[5] thigh[6] and hip,[7] eluding accurate diagnosis for long periods. In our case also, there were several medical and orthopaedic consultations in three years for the pain. In such cases, a high index of clinical suspicion is required for diagnosis of glomus tumour. Multiple glomus tumours and involvement of internal organs have also been reported.
Interestingly, the variation in anatomic site of tumor has a striking relation to the sex of the patient. Tsuneyoshi and Enjoji,[8] in their study of 63 patients of glomus tumours, observed that out of the 37 patients with the tumour in a finger or a toe, 34 were women and only three were men and of the 26 patients with the tumours in other area, 19 were men and only seven were women. So men are more likely to have extradigital location, as was seen in our case.
Histologically, the tumours have variable quantities of glomus cell, blood vessels and smooth muscles.[9] According to this observation, they are classified as solid glomus tumour, glomangioma and glomangiomyoma. Solid glomus tumour is composed of solid aggregates of glomus cells surrounding inconspicuous vessels. Glomus cells are round regular cells with eosinophilic cells and dark staining round to oval nuclei. Glomangiomas have more prominent vessels and less conspicuous glomus cells. Some tumours may show a transition from glomus cells to smooth muscle cells. They have been called glomangiomyoma. Simple excision is curative with a low recurrence rate.
The present case illustrates the importance of keeping a high index of clinical suspicion for the diagnosis of glomus tumour, occurring in an extradigital site. Accurate diagnosis can only be made if appropriate physical findings are looked for, especially in locations where the tumor occurs less commonly. It also reiterates the fact that for clinical diagnosis of a dermatosis, clinical signs and symptoms give the most important clue though distribution may be unusual.
| 1. |
Shugart RR, Soule EH, Johnson EW Jr. Glomus tumor. Surg Gynecol Obstet 1963;117:334-40.
[Google Scholar]
|
| 2. |
Walsh JJ, Eady JL. Vascular tumors. Hand Clin 2004;20:261-8.
[Google Scholar]
|
| 3. |
Smyth M. Glomus cell tumors in the lower extremity. Reports of two cases. J Bone Joint Surg Am 1971;53:157-9.
[Google Scholar]
|
| 4. |
Quigley JT. A glomus tumor of the heel pad. A case report. J Bone Joint Surg Am 1979;61:443-4.
[Google Scholar]
|
| 5. |
Coughey DE, Highton TC. Glomus tumor of the knee. J Bone Joint Surg Br 1966;48:134-7.
[Google Scholar]
|
| 6. |
Negri G, Schulte M, Mohr W. Glomus tumor with diffuse infiltration of the quadriceps muscle. A case report. Hum Pathol 1997;28:750-2.
[Google Scholar]
|
| 7. |
Gencosmanoglu R, Inceoglu R, Kurtkaya-Yapicier O. Glomangioma of the hip. Dermatol Surg 2003;29:1244-7.
[Google Scholar]
|
| 8. |
Tsuneyoshi M, Enjoji M. Glomus tumor. A clinicopathologic and electron microscopic study. Cancer 1982;50:1601-7.
[Google Scholar]
|
| 9. |
Weedon D. Vascular tumors. In : Weedon D. ed. Skin Pathology, 2nd edn. London: Churchill Livingstone; 2002. p. 1016-7.
[Google Scholar]
|
Fulltext Views
2,127
PDF downloads
2,918





![[Figure - 1]](#fig_ijdvl_2006_72_4_327_26716_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2006_72_4_327_26716_2.jpg){kind=link}