Translate this page into:
Linear cord-like lesion on the chest wall
Correspondence Address:
Mary Muthachen
C4C Willingdon Enclave, Thevera, Kochi 682 013, Kerala
India
| How to cite this article: Muthachen M. Linear cord-like lesion on the chest wall. Indian J Dermatol Venereol Leprol 2006;72:252 |
 |
|
 |
|
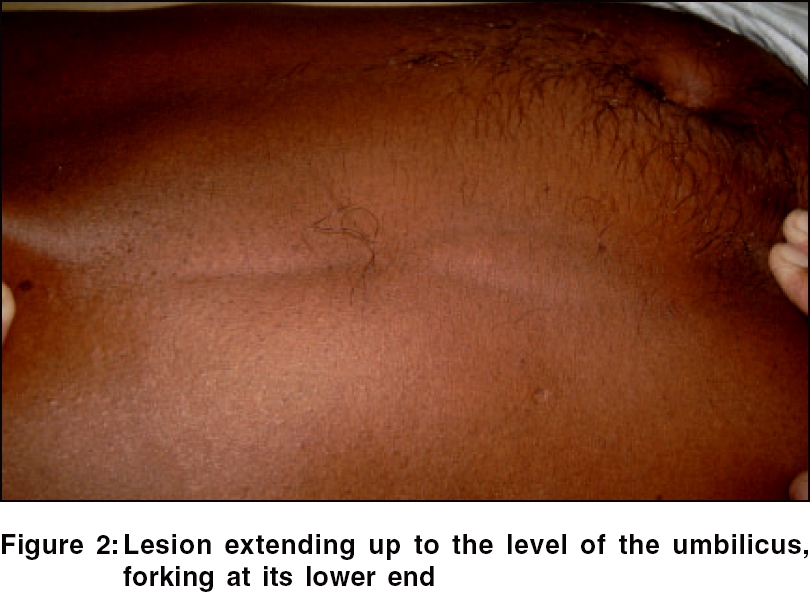
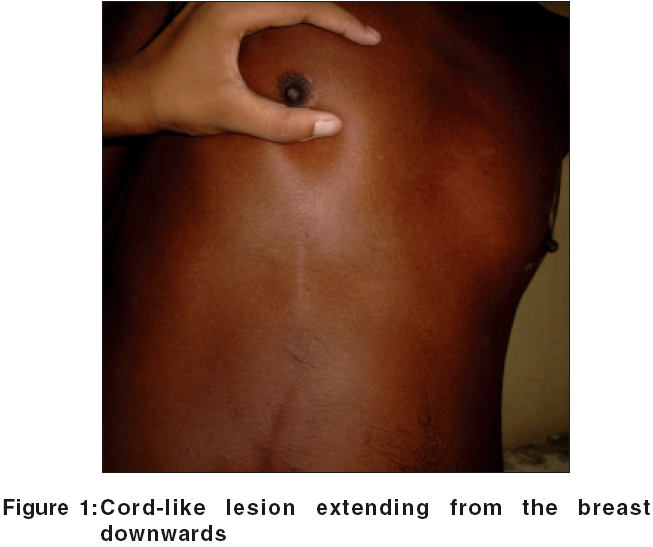
A 53-year-old male patient, a laborer by profession, presented with a 3-week history of a cord-like lesion on the anterior chest wall. On examination, there was a skin-colored linear cord starting from the inferolateral quadrant of the right breast, crossing the lower margin of the rib cage on the same side and ending at a level just above the umbilicus [Figure - 1]. In its lower part, the cord forked and took on an inverted-V shape. It was about 3 mm in width and about 25 cm in length. It was attached to the skin but not to the subcutaneous tissue. On stretching the skin, a shallow groove became apparent alongside the cord [Figure - 2]. Examination of the breast and axillary region did not reveal any palpable masses.
A routine hematology work-up and an ultrasound scan were normal. A mammogram was reported as showing no evidence of spiculated mass lesions or suspicious microcalcifications.
What is the diagnosis?
Diagnosis: Mondor′s disease or sclerosing periphlebitis of the chest wall
Discussion
Mondor′s disease is named after Henri Mondor (1885-1960), a French surgeon, who in 1939 was the first to fully describe this condition - namely, a thrombophlebitis generally affecting the thoracoepigastric, lateral thoracic or the superficial epigastric veins.[1] It is an uncommon condition. Incidence rates of 0.84 to 0.96% have been reported. It occurs three times as frequently in women as in men, generally in the age group of 30 to 60 years. The sudden appearance of a rope-like band along the anterior chest wall is characteristic. Erythematous and tender at first, it thereafter changes into a painless tough cord-like strand. Both sides of the chest have the same incidence of involvement.[2] Rarely, the condition is bilateral. Many reasons have been ascribed to its onset and development - strenuous exercise, trauma, infection near the affected vessels, stereotactic vacuum assisted biopsy of the breast, underlying overt or occult malignant disease of the breast, tight clothing, pregnancy and a large pendulous breast.[1],[2],[3]
It has been postulated that direct trauma to the veins, or pressure on the lateral thoracic veins leading to stasis of blood may be the cause. In other cases, the most reasonable explanation is on the basis of repeated movement of the breast along with contracting and relaxing pectoral muscles, which cause stretching and relaxing of the veins.[4] A majority of biopsied lesions show a subcutaneous vein with organizing thrombi and fibrous thickened walls.[5]
Mammographic findings are of a tubular density, along with a sonographic finding of a superficial vessel with or without an intraluminal thrombus. A tubular anechoic structure with multiple areas of narrowing giving a beaded appearance to the vessel and without flow on Doppler Imaging are the typical findings of Mondor′s disease.[6] Mammogram may however be unremarkable, as in this patient.
The course of the disease is uneventful. There is no increased risk of blood clots in other veins. The condition subsides within 2-8 weeks, leaving no traces or complications in its aftermath. Treatment is symptomatic and as the discomfort is minor, warm compresses and analgesics will generally suffice.
Thus, while generally being a benign and self-limiting condition, the physician should be aware that Mondor′s disease might occasionally be the presenting symptom of breast cancer. Appropriate investigations to rule out this possibility must be conducted.
| 1. |
Jaberi M, Willey S, Bremm R. Stereotactic vacuum assisted Breast biopsy-An unusual cause of Mondor's disease. Am J Roentgenol 2002;179:185-6.
[Google Scholar]
|
| 2. |
Cutaneous Vascular diseases. In : Odom RB, James WD, Berger TG editors. Andrews' Diseases of the skin - Clinical Dermatology. 9th ed. WB Saunders: Philadelphia; 2000. p. 1026.
[Google Scholar]
|
| 3. |
Burns DA. The Breast. In : Champion RH, Burton JL, Burns DA. Breathnach SM, editors. Rook/ Wilkinson/ Ebling Textbook of dermatology. 6th ed. Blackwell Science: Oxford; 1998. p. 67.15-6.
[Google Scholar]
|
| 4. |
Hogan GF. Mondor's disease. Arch Intern Med 1964;113:881-5.
[Google Scholar]
|
| 5. |
Barnhill R, Busam K. Vascular diseases. In : Elder D, Elenitsas R, Jaworsky C, Johnson B, editors. Lever's Histopathology of the skin. 8th ed. Lippincott-Raven: Philadelphia; 1997. p. 192-3.
[Google Scholar]
|
| 6. |
Shetty MK, Watson AB. Mondor's disease of the breast: sonographic and Mammographic findings. Am J Roentgenol 2001;177:893-6.
[Google Scholar]
|
Fulltext Views
4,237
PDF downloads
1,843





![[Figure - 1]](#fig_ijdvl_2006_72_3_252_25801_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2006_72_3_252_25801_2.jpg){kind=link}