Translate this page into:
Spontaneous partial repigmentation of halo nevi around congenital melanocytic nevus and vitiligo in a 13-year-old boy
2 Hospital del Ni�o Jes�s, Madrid, Spain
3 Complejo Hospitalario Universitario de Albacete, Albacete, Spain
4 Complexo Hospitalario de Pontevedra, Pontevedra, Spain
Correspondence Address:
M J Concha-Garz�n
C/ Diego de le�n 62, CP 28006, Madrid
Spain
| How to cite this article: Concha-Garz�n M J, Hern�ndez-Mart�n A, Faura-Berruga C, D�vila-Seijo P, Torrelo A. Spontaneous partial repigmentation of halo nevi around congenital melanocytic nevus and vitiligo in a 13-year-old boy. Indian J Dermatol Venereol Leprol 2014;80:69-70 |
Sir,
Halo nevi (HN) or leukoderma acquisitum centrifugum is a ring of depigmentation that may appear around acquired or congenital melanocytic nevi (CMN) as well as melanoma. In some cases, the hypopigmented halo anticipates the total or partial regression of the melanocytic lesion, while in others it remains stable or eventually undergoes repigmentation. [1] HN is not uncommon, being more frequent around acquired melanocytic nevus. [2] Up to 26% of patients with HN have vitiligo, [3] but in very few instances is there an association of HN around CMN and vitiligo. [4] The exact mechanisms responsible for the development of vitiligo and HN and its resolution are unknown. One of the most accepted hypotheses considers that both phenomena are a result of a self-limited immunologic response to pigmented cells, either in the "′normal"′ skin or within the melanocytic lesion. [4] We report a case of halo CMN that subsequently developed vitiligo and spontaneous partial repigmentation of both lesions.
A 2-week-old Caucasian male came to our clinic for evaluation of a congenital pigmented lesion on the right knee. On physical examination, there was a 3 × 1.5 cm dark brown melanocytic lesion noted. Histopathologic study confirmed a compound CMN and the patient was scheduled for periodic follow-up. The lesion remained stable until the patient was 6 years old; at that time, a hypopigmented halo and partial regression of the lesion was observed. Ten months later, the patient developed achromic macules on the sacral region and both ankles consistent with vitiligo. There was no family history of vitiligo, melanoma, or autoimmune diseases. Treatment with tacrolimus 0.1% ointment for 3 months was ineffective. A year later, the sacral lesion and the halo started to show partial repigmentation while the ankle depigmentation remained stable. When the child was 13 years old, vitiligo lesions of the lower extremities began to show spontaneous resolution, parallel to progressive repigmentation of the halo and complete resolution of the sacral lesion [Figure - 1].
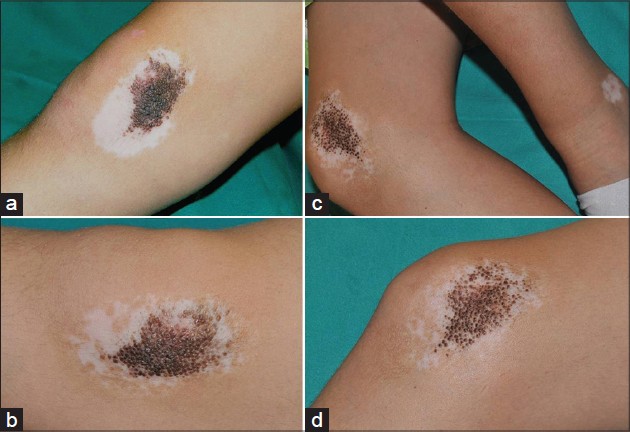 |
| Figure 1: (a) Halo CMN on the inner aspect of the right knee when the patient was 8 years old. (b) Follow-up at the age of 10 years. Partial regression of the CMN is observed, as well as patchy areas of repigmentation. (c and d) Substantial repigmentation both halo CMN and vitiligo when the patient was 13 years old |
The occurrence of halo CMN is a well-known phenomenon, as is its association with vitiligo, [1],[2],[3],[4],[5] but halo repigmentation in congenital melanocytic lesions is exceptional. [4] We have found only two more cases in the literature: A 2-year-old boy with a CMN on the arm who experienced total regression of the CMN and partial repigmentation [5] and another case included in a series of cases of halo CMN and vitiligo in which some repigmentation was observed at the periphery. [4] Additionally, in a series of 52 patients with HN in which no differentiation between acquired and congenital lesions was made, the authors state that partial or complete repigmentation of the HN was observed after an average follow-up of 11.8 and 7.8 years, respectively, [1] so it is possible that repigmentation may occur later in life and regression of HN in all CMN is a question of time. Management of CMN with halo does not differ from cases without peripheral depigmentation, and periodic follow-up is recommended unless worrisome changes occur. In conclusion, it is important to recognise the possibility of spontaneous repigmentation in cases of halo CMN and the associated vitiligo.
| 1. |
Aouthmany M, Weinstein M, Zirwas MJ, Brodell RT. The natural history of halo nevi: A retrospective case series. J Am Acad Dermatol 2012;67:582-6.
[Google Scholar]
|
| 2. |
Kim HS, Goh BK. Vitiligo occurring after halo formation around congenital melanocytic nevi. Pediatr Dermatol 2009;26:755-6.
[Google Scholar]
|
| 3. |
Stierman SC, Tierney EP, Shwayder TA. Halo congenital nevocellular nevi associated with extralesional vitiligo: A case series with review of the literature. Pediatr Dermatol 2009;26:414-24.
[Google Scholar]
|
| 4. |
Guerra-Tapia A, Isarría MJ. Periocular vitiligo with onset around a congenital divided nevus of the eyelid. Pediatr Dermatol 2005;22:427-9.
[Google Scholar]
|
| 5. |
Kikuchi I, Inoue S, Ogata K, Idemori M. Disappearance of a nevocellular nevus with depigmentation. Arch Dermatol 1984;120:678-9.
[Google Scholar]
|
Fulltext Views
4,593
PDF downloads
3,353





![[Figure - 1]](#fig_ijdvl_2014_80_1_69_125539_f1.jpg){kind=link}