Translate this page into:
Successful use of imiquimod 5% cream in Bowen's disease
2 Department of Pathology, Kasturba Medical College, Manipal, India
Correspondence Address:
Smitha Prabhu
Department of Skin and STD, KMC, Manipal
India
| How to cite this article: Prabhu S, Rao R, Sripathi H, Hameed S, Kuduva R. Successful use of imiquimod 5% cream in Bowen's disease. Indian J Dermatol Venereol Leprol 2007;73:423-425 |
 |
| Figure 4: Atrophic epidermis and a normal dermis at 24 weeks (H and E stain, x100) |
|
| Figure 4: Atrophic epidermis and a normal dermis at 24 weeks (H and E stain, x100) |
 |
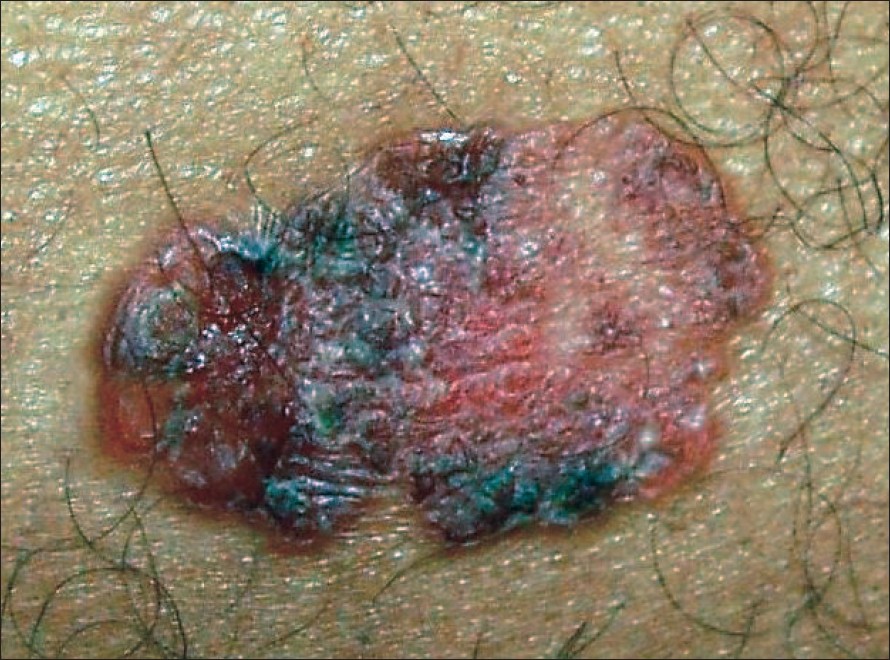
| Figure 3: Clinical improvement at 24 weeks follow-up with atrophy and pigmentation |
|
| Figure 3: Clinical improvement at 24 weeks follow-up with atrophy and pigmentation |
 |
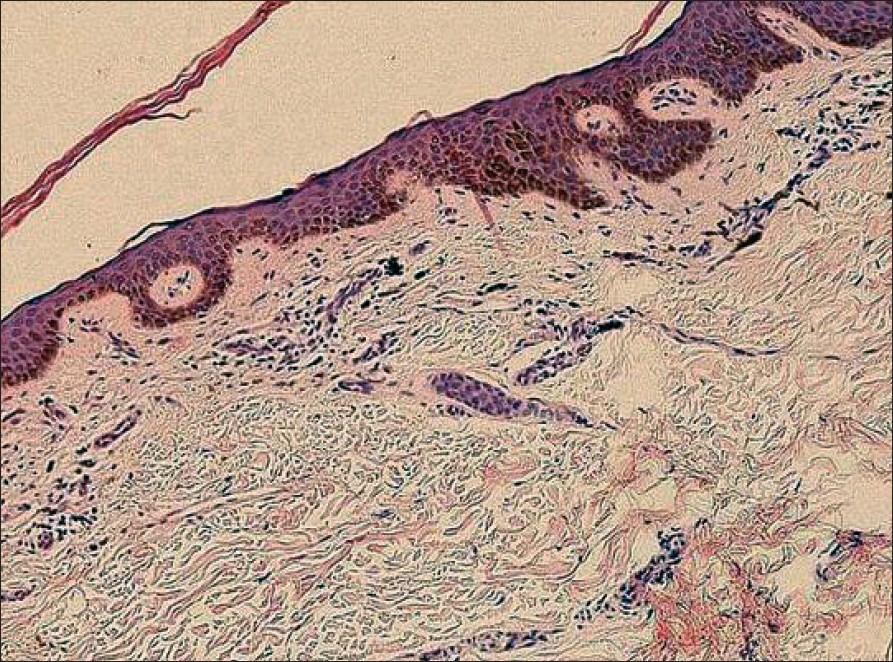
| Figure 2: Atypical keratinocytes with mitotic figures in a windblown appearance, limited to the epidermis (H and E stain, x400,) |
|
| Figure 2: Atypical keratinocytes with mitotic figures in a windblown appearance, limited to the epidermis (H and E stain, x400,) |
 |
| Figure 1: Erythematous scaly plaque, 5 x 3 cm, over right thigh with erosion and crusting at places |
|
| Figure 1: Erythematous scaly plaque, 5 x 3 cm, over right thigh with erosion and crusting at places |
Sir,
Bowen′s disease is a rare, persistent, progressive intraepidermal carcinoma, which may be potentially malignant, with up to 8% of the cases progressing to squamous cell carcinoma. The various treatment modalities include physical destruction using electrocautery, cryotherapy, curettage, laser therapy or surgical excision, intralesional interferon alpha or bleomycin and noninvasive methods like photodynamic therapy and topical 5-fluorouracil. Most of these therapies are administered by the physician, rather than being self-administered. Imiquimod is a topical immune response modifier with antitumor and antiviral activity. Its utility in Bowen′s disease, including penile, facial, vulvar, truncal and recurrent nail disease has been reported by many authors. Here we report its successful use in an Indian patient with Bowen′s disease.
A 45 year-old male factory worker presented to us with a persistent, occasionally itchy, progressively enlarging psoriasiform plaque of six months′ duration measuring 5 x 3 cm, on the right thigh [Figure - 1]. It had not responded to topical steroids, salicylic acid, coal tar, retinoids or tacrolimus. With a differential diagnosis of Bowen′s disease and lupus vulgaris, a skin biopsy was done and it revealed the features of Bowen′s disease [Figure - 2]. He was started with 5% topical imiquimod, which was applied to the plaque on three alternate days in a week, with monthly follow-up. The lesion progressively decreased in size and thickness at each follow-up. At the three-months′ follow-up, the lesion had totally flattened with persisting hyperpigmentation. A repeat biopsy at this stage revealed a normal epidermis. Imiquimod was stopped and the patient was advised follow-up every three months. After six months, the lesion had completely cleared with atrophy and pigmentation [Figure - 3] and a third biopsy done at this stage was also clear [Figure - 4]. The patient is still under follow-up at six monthly intervals, but there has been no recurrence of the lesion at the end of one year.
Imiquimod is a potent antiviral and antitumor agent, approved by the US FDA as a topical agent in the treatment of genital and perianal warts. [1] It was later found to be beneficial in a number of cutaneous disorders including many viral infections and malignant as well as premalignant conditions, including Bowen′s disease.
In a phase II trial by Mackenzie-Wood et al , the first open labeled study evaluating the use of imiquimod in Bowen′s disease, a once daily application of 5% imiquimod for 16 weeks was found to be effective in 14 out of 15 patients. [2] In a randomized, double-blind, placebo-controlled trial involving 34 patients with Bowen′s disease, out of 15 patients who were treated with imiquimod 5% cream, 11 achieved resolution of their lesions with no relapse during a follow-up period of nine months. [3] A phase II, randomized, double-blind, vehicle-controlled trial involving 129 patients with histologically proven basal cell carcinoma gave complete response rates of 100, 87.1, 80.8 and 51.7% for patients in twice daily, once daily, five times a week and 3 times a week dosage schedules of 5% imiquimod, respectively. [4]
Various regimes of topical treatment of cutaneous malignancies with imiquimod include alternate nights to twice daily application from a minimum of six weeks to a maximum of 20 weeks. [2],[3],[4] The more frequent the application, the greater the chance for application site reactions, which occur at a frequency of 1% and include pruritus, burning, soreness, erythema, scabbing, flaking, erosion, crusting, edema and induration, which are usually mild-moderate and are dose-dependent. A thrice weekly regime is recommended in most studies because it is the least aggressive treatment which gives the greatest success rate, nearly approaching 100%.
We preferred imiquimod 5% cream over other modalities of treatment because of the easy availability, ease of self administration, lack of pain, and lack of need for hospitalization and the encouraging reports published in the last few years.
| 1. |
Sauder DN. Immunomodulatory and pharmacologic properties of Imiquimod. J Am Acad Dermatol 2000;43:S6-11.
[Google Scholar]
|
| 2. |
Mackenzie-Wood A, Kossard S, de Launey J, Wilkinson B, Owens ML. Imiquimod 5% cream in the treatment of Bowen's disease. J Am Acad Dermatol 2001;44:462-70.
[Google Scholar]
|
| 3. |
Patel GK, Goodwin R, Chawla M, Leidler P, Price PE, Finlay AY, et al . Imiquimod 5% cream monotherapy for cutaneous squamous cell carcinoma in-situ (Bowen's disease): A randomized, double-blind, placebo-controlled trial. J Am Acad Dermatol 2006;54:1025-32.
[Google Scholar]
|
| 4. |
Geisse JK, Rich P, Pandya A, Gross K, Andres K, Ginkel A, et al . Imiquimod 5% cream for the treatment of superficial basal cell carcinoma: A double-blind, randomized, vehicle-controlled study. J Am Acad Dermatol 2002;47:390-8.
[Google Scholar]
|
Fulltext Views
3,794
PDF downloads
2,085





![[Figure - 1]](#fig_ijdvl_2007_73_6_423_37066_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2007_73_6_423_37066_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2007_73_6_423_37066_3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2007_73_6_423_37066_4.jpg){kind=link}