Translate this page into:
Symmetrical erythematous annular and scaly patches
Correspondence Address:
Najeeba Riyaz
Arakkal Chalapuram, Calicut - 673002, Kerala
India
| How to cite this article: Riyaz N, Rajan U, Anuradha K B. Symmetrical erythematous annular and scaly patches. Indian J Dermatol Venereol Leprol 2007;73:446 |
 |
| Figure 4: Improvement of skin lesions after surgery |
|
| Figure 4: Improvement of skin lesions after surgery |
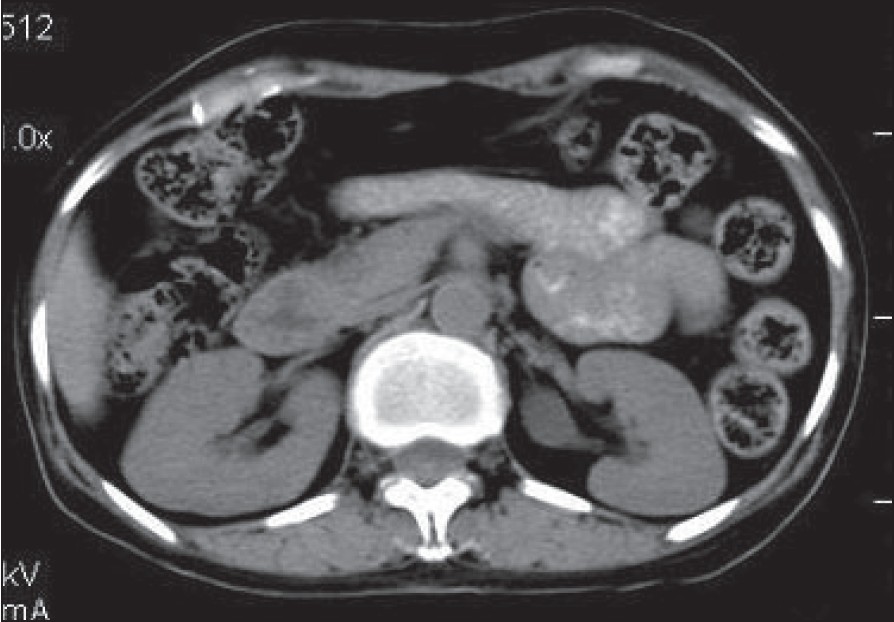 |
| Figure 3: CT scan of the abdomen showing a well-enhanced, soft tissue lesion 56 x 40 x 30 mm in size with a speck of calcification in the tail of the pancreas |
|
| Figure 3: CT scan of the abdomen showing a well-enhanced, soft tissue lesion 56 x 40 x 30 mm in size with a speck of calcification in the tail of the pancreas |
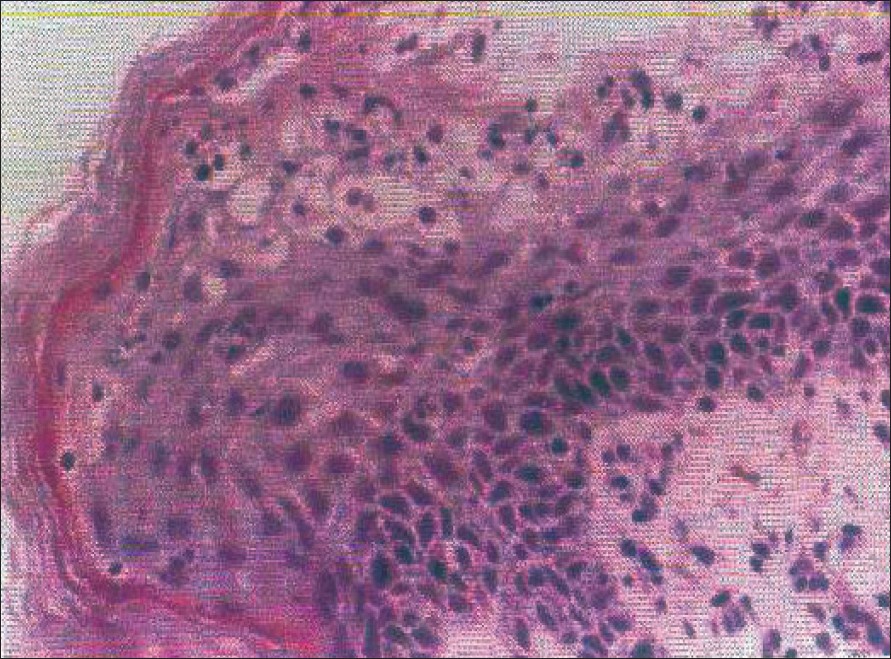 |
| Figure 2: Intraepidermal cleft and vacuolated pale epidermal cells (H and E, x400) |
|
| Figure 2: Intraepidermal cleft and vacuolated pale epidermal cells (H and E, x400) |
 |
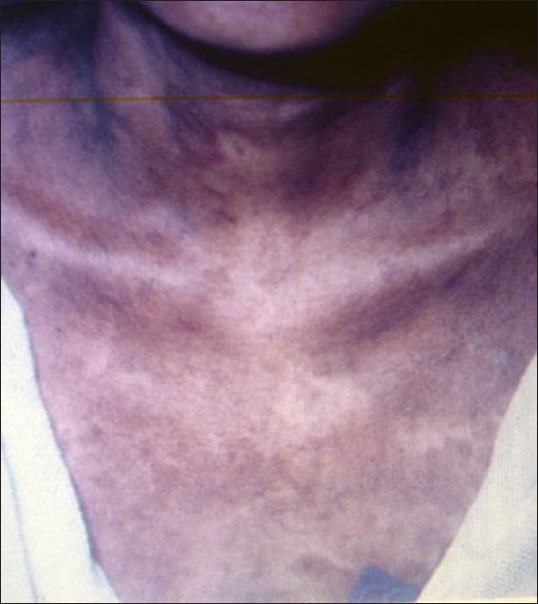
| Figure 1: Erythematous scaly annular and serpiginous plaques with areas of erosions and pigmentation on the trunk |
|
| Figure 1: Erythematous scaly annular and serpiginous plaques with areas of erosions and pigmentation on the trunk |
A 52 year-old woman presented with a two-year history of pruritic, burning and expanding red rings involving the entire body. She had marked fatigue, anorexia and weight loss. Examination revealed a cachectic woman with symmetrical erythematous annular and scaly patches involving the trunk [Figure - 1], lower limbs and back. A few pustules and vesicles were present on the trunk. Intertriginous areas showed erosions. Glossitis and stomatitis were also present.
Investigations revealed a hemoglobin (Hb) value of 7.5 gm%, hyperglycemia (postprandial blood sugar, PPBS = 320 mg%), abnormal glucose tolerance test results and aminoaciduria. Skin biopsy showed intraepidermal cleft, vacuolated pale epidermal cells with pyknotic nuclei and neutrophils in the upper epidermis [Figure - 2].
What is your Diagnosis ?

| 1. |
Sweet RD. A dermatosis specifically associated with tumour of pancreatic alpha cells. Br J Dermatol 1974;90:301-8.
[Google Scholar]
|
| 2. |
Wilkinson DS. Necrolytic migratory erythema with pancreatic carcinoma. Proc R Soc Med 1971;64:1197-8.
[Google Scholar]
|
| 3. |
Marinkovich MP, Botella R, Datloff J, Sangueza OP. Necrolytic migratory erythema without glucagonoma in patients with liver disease. J Am Acad Dermatol 1995;32:605-9.
[Google Scholar]
|
| 4. |
Blacford S, Wright S, Roberts DL. Necrolytic migratory erythema without glucagonoma: The role of dietary essential fatty acids. Br J Dermatol 1991;125:460-2.
[Google Scholar]
|
| 5. |
Kelly CP, Johnson CF, Nolan N, Keeling PW, Weir DG. Necrolytic migratory erythema with elevated plasma enteroglucagon in celiac disease. Gastroenterology 1989;96:1350-3.
[Google Scholar]
|
| 6. |
Mullans EA, Cohen PR. Iatrogenic necrolytic migratory erythema. A case report and review of non-glucagonoma associated necrolytic migratory erythema. J Am Acad Dermatol 1998;38:866-73.
[Google Scholar]
|
| 7. |
Peterson LL, Shaw JC, Acott KM, Mueggler PA, Parker F. Glucagonoma syndrome: In vitro evidence that glucagon increases epidermal arachidonic acid. J Am Acad Dermatol 1984;11:468-73.
[Google Scholar]
|
| 8. |
Bewly AP, Ross JS, Bunker CB, Staughton RC. Successful treatment of a patient with octreotide-resistant necrolytic migratory erythema. Br J Dermatol 1996;134:1101-4.
[Google Scholar]
|
| 9. |
van der Loos TL, Lambrecht ER, Lambers JC. Successful treatment of glucagonoma related necrolytic migratory erythema with dacarbazine. J Am Acad Dermatol 1987;16:468-72.
[Google Scholar]
|
Fulltext Views
2,937
PDF downloads
2,694





![[Figure - 1]](#fig_ijdvl_2007_73_6_446_37083_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2007_73_6_446_37083_2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2007_73_6_446_37083_3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2007_73_6_446_37083_4.jpg){kind=link}