
Translate this page into:
The ping-pong infection in gonorrhoea: Lest we forget
Corresponding author: Dr. Somesh Gupta, Professor, Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi, India. someshgupta@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Dev T, Mahajan N, Sood S, Gupta S. The ping-pong infection in gonorrhoea: Lest we forget. Indian J Dermatol Venereol Leprol 2022;88:109-11.
Sir,
Contact tracing in sexually transmitted infections is often understated. We describe a related entity, “the ping-pong” infection in gonococcal urethritis.
A 26-year-old unmarried man, working as ground staff at the airport, presented with dysuria and discharge per urethra for five days with no systemic symptoms. A few days ago, he had sexual contact with a female sex worker. Besides, he was in a regular non-marital sexual relationship (unprotected) for the past six months with a married woman, whose husband was an army personnel. Both the partners, however, were asymptomatic.
There was profuse discharge per urethra which was foul-smelling, greenish, thick, purulent and associated with perimeatal erythema. There was no inguinal lymphadenopathy. Gram smear of the discharge revealed abundant polymorphonuclear cells along with both intra and extracellular Gram-negative diplococci. A diagnosis of gonococcal urethritis was made which was confirmed by nucleic acid amplification test. An in-house opa gene and the porA pseudogene-based polymerase chain reaction assay were used for confirmation. Culture on modified Thayer Martin and chocolate agar medium was also done. The suspected colonies in culture were confirmed by Gram stain as well as oxidase, superoxol and rapid carbohydrate utilization tests. Antimicrobial susceptibility test of Neisseria gonorrhoeae isolates was done by disc diffusion method, minimum inhibitory concentration (MIC) was determined by E test and the results were interpreted using the breakpoint criteria of calibrated dichotomous sensitivity technique.1
Low concentration antibiotic discs (Oxoid Basingstoke, UK) which included penicillin (0.5 IU), ciprofloxacin (1 microgram), nalidixic acid (30 μg), ceftriaxone (0.5 μg), cefpodoxime (10 micrograms), spectinomycin (100 μg), tetracycline (10 micrograms) and azithromycin (15 µg) were used. In addition, cefixime (5 micrograms) was tested and interpreted as per the Clinical and Laboratory Standards Institute (CLSI) guidelines.2 The strain was susceptible to ceftriaxone (annular radius – 14 mm; MIC – 0.003 μg/ml), cefpodoxime, azithromycin (annular radius – 16 mm; MIC – 0.094 μg/ml) and spectinomycin. Cefpodoxime was used as a surrogate marker for oral cephalosporins. It exhibited high-level resistance to ciprofloxacin and plasmid-mediated high-level resistance to tetracycline (tetracycline-resistant Neisseria gonorrhoeae). It was penicillinase-producing Neisseria gonorrhoeae (PPNG) strain. Polymerase chain reaction and culture were negative for Ureaplasma urealyticum, Mycoplasma hominis, Mycoplasma genitalium and Chlamydia trachomatis. Serology for human immunodeficiency virus infection and syphilis (Venereal Disease Research Laboratory test) was negative.
The patient and regular partner received single intramuscular injection of ceftriaxone (250 mg) and azithromycin one gram stat (per oral) and counselling for safe sex. All symptoms resolved in a week. The sex worker could not be contacted.
Three weeks later, the patient reconsulted with same complaints. The re-occurrence of the symptoms and demonstration of Gram-negative intracellular diplococci prompted a diagnosis of reinfection with Neisseia gonorrhoeae. The index case had sexual contact with the regular partner during the intervening period, who also had sexual contact with her husband, who returned home briefly before she received the treatment. The index patient denied any other contact during this period. The woman’s husband could not be treated as she refused to inform him because of the risk of marital discord. Neisseria gonorrhoeae multiantigen sequence typing of isolates during the two episodes revealed identical sequence type with ST556.This complex chain of transmission can be described as ping-pong infection [Figure 1].3
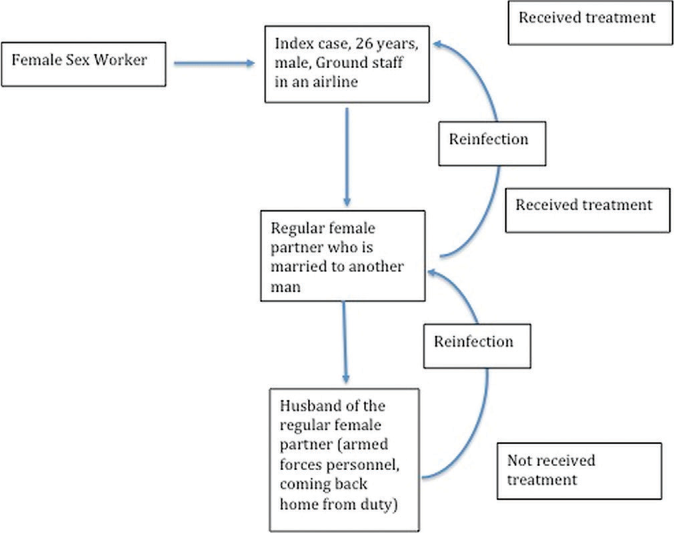
- A flow diagram depicting the ping-pong phenomenon. The index case got infection from a female sex worker and transmitted to his regular non-marital partner, who further spread it to her husband. After diagnosis of gonorrhea, the index case and his female partner received treatment; however, the husband could not be treated. The female partner reacquired the infection from her untreated husband and eventually brought it back to the index case
Sexually transmitted infections involve a cobweb of patients, carriers and susceptible individuals. The number of partners, hetero/homosexual contact, protected/unprotected act, influence of alcohol and drugs and exposure to sex workers influence the course of infections. It is compounded when multiple sex partners are involved which complicates contact tracing and motivating them to pursue clinical evaluation. Modern tools such as e-mail, SMS or WhatsApp can be utilized to bridge the psychological and physical distance between the susceptible contacts and health-care facility while maintaining confidentiality and anonymity.4,5 The barrier to contact tracing, however, is the fear of sociocultural implications of having multiple sexual partners including marital disharmony and intimate partner violence.
Detailed sexual history, clinical examination and bedside laboratory investigation are essential.6 Dual therapy with intramuscular injection of ceftriaxone (250 mg) and one gram azithromycin per oral improves treatment efficacy, reduces drug resistance and provides coverage against coinfection with Chlamydia trachomatis.7 Needless to say, antibiotics do not offer additional immunity/protection from reinfection, hence, the risk of reinfection in case of continued high-risk behavior is certainly high. The identical genotype of the isolates during both the episode of urethral discharge indicates that the index case suffered “ping-pong” infection through the complex chain of transmission [Figure 1] with the same genotype of Neisseria gonorrhoeae.
Due to the short incubation period, high infectivity and acute clinical presentation, ping-pong phenomena in gonococcal infection provides a vivid glimpse into the consequences of unprotected sex with multiple partners and emphasizes the importance of protected sex and partner management.3
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 2011. (Sixth Edition). :45-49. Antibiotic Reference Laboratory, South Eastren Area Laboratory Sercivices. Available http://cdstest.net
- [Google Scholar]
- A pilot study to determine Neisseria gonorrhoeae-chlamydia trachomatis coinfection rates in symptomatic patients attending STI Clinics, New Delhi, India. Indian J Dermatol Venereol Leprol. 2021;87:1-5.
- [CrossRef] [PubMed] [Google Scholar]
- Ping-pong effect In: Kirch W, ed. Encyclopedia of Public Health. Berlin, Germany: Springer; 2008.
- [Google Scholar]
- Expedited partner therapy for sexually transmitted diseases-are we there yet? Sex Transm Dis. 2014;41:695-7.
- [CrossRef] [PubMed] [Google Scholar]
- Follow the sex: Influence of network structure on the effectiveness and cost-effectiveness of partner management strategies for sexually transmitted infection control. Sex Transm Dis. 2020;47:71-9.
- [CrossRef] [PubMed] [Google Scholar]
- Recalibrating the gram stain diagnosis of male urethritis in the era of nucleic acid amplification testing. Sex Transm Dis. 2012;39:18-20.
- [CrossRef] [PubMed] [Google Scholar]
- Sexually Transmitted Diseases Treatment Guidelines, U.S. Department of Health and Human Services. 2015. Centers for Disease Control and Prevention. Available from: https://www.cdc.gov/std/tg2015/gonorrhea.html [Last accessed on 2020 Nov 18]
- [Google Scholar]




