Translate this page into:
Tinea corporis due to Trichophyton mentagrophytes and Trichophyton tonsurans mimicking tinea imbricata
Correspondence Address:
Angoori Gnaneshwar Rao
F12 B 8 HIGII, APHB Baghlingampally, Hyderabad, AP
India
| How to cite this article: Rao AG, Datta N. Tinea corporis due to Trichophyton mentagrophytes and Trichophyton tonsurans mimicking tinea imbricata. Indian J Dermatol Venereol Leprol 2013;79:554 |
Sir,
Dermatophytoses due to Trichophyton mentagrophytes (TM) and Trichophyton tonsurans (TT) clinically manifest as erythematous annular plaques or patches with papules or vesicles at the margin. However, they may rarely present with multiple concentric rings with in the plaque resembling tinea imbricate (TI) caused by Trichophyton concentricum. [1]
A 35-day-old baby (case 1) was brought with annular erythematous scaly patch on the left lateral wall of the chest and 22-year-old lady (case 2) presented with annular scaly patch on left shoulder. Family history was negative for dermatomycosis in both the cases and there was no history of any topical application. Case 1 was under treatment for protein energy malnutrition (PEM). Both were found to have single erythematous, circumscribed patch; on the left lateral wall of the chest in case 1 and on the left shoulder in case 2 [Figure - 1]. There were two concentric rings of scales within the plaque in both the cases. Hair and nails were normal in them. TI was provisionally diagnosed based on the typical morphology of the lesions. However, Tinea corporis, erythema annulare centrifugum, granuloma annulare were considered in the differential diagnosis. Potassium hydroxide (KOH) mount of the scrapings taken from the margins of both concentric rings from both patients showed numerous irregular, branched and septate hyphae [Figure - 2]. Culture on Sabouraud′s dextrose agar in case 1 showed creamish white colony with granular surface and raised center [Figure - 2]; reverse showed yellow-brown pigmentation) consistent with TM; culture in case 2 showed yellow, powdery, flat colonies with radial grooves and reverse reddish brown pigmentation consistent with TT. Trichophytin intradermal test could not be done in both the cases. Both were managed with 1% clotrimazole cream topically for 3 weeks which relieved their symptoms.
Both TM and TT are ubiquitous fungi. Both dermatophytes cause tinea capitis and most likely cause T. corporis. Interestingly the prevalence of T. corporis caused by TM and TT is increasing. [2]
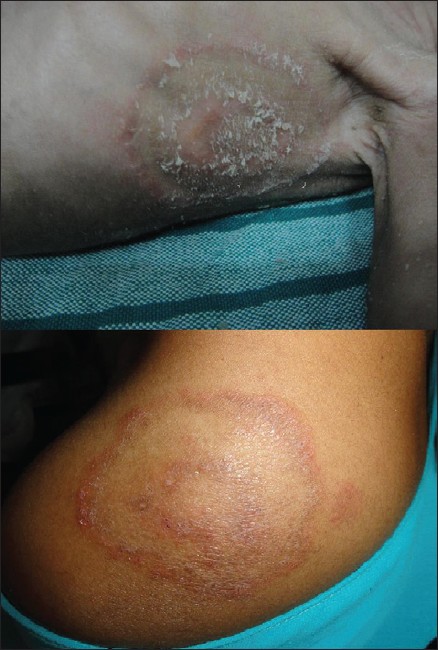 |
| Figure 1: Upper picture showing annular plaque on the left lateral wall of the chest with concentric ring. Lower picture showing annular plaque with central ring of scales on the left shoulder region |
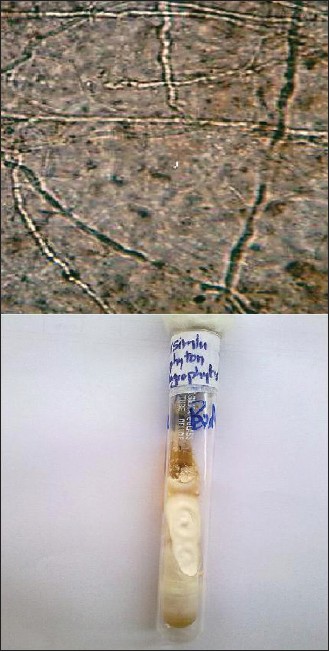 |
| Figure 2: Upper picture Potassium hydroxide preparation of scrapings showing numerous irregular, branched and septate hyphae (×40). Lower picture Culture on Sabouraud's dextrose agar showing creamish white colony with granular surface and raised center, characteristic of Trichophyton mentagrophytes |
Although, numerous concentric rings is a characteristic feature of TI, a second wave of centrifugal spread may infrequently occur from initial site with formation of 1 or 2 concentric rings in annular T. corporis. It was thought that villous hair in the involved area may be invaded and the follicle acts as a reservoir of infection. [1]
It is known that PEM is associated with significant impairment of cell mediated immunity (CMI), phagocyte function, complement system, immunoglobulin A and cytokine production. [3] Consequently patients with PEM show consistent impairment of cutaneous delayed hypersensitivity and fewer circulating T lymphocytes. [4]
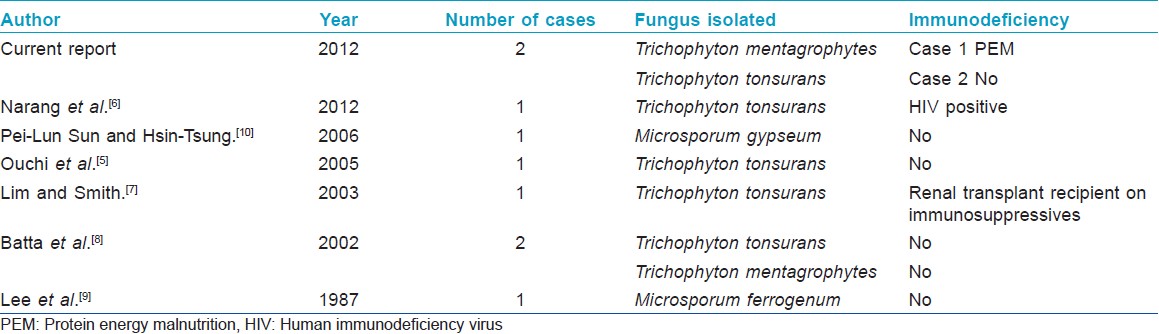
The case 1 under study is a case of PEM ; the clinical morphology (concentric rings) due to TM mimicking TI may be explained by the apparent impairment of CMI due to PEM. Review of literature revealed three similar cases reported as tinea pseudoimbricata or tinea indecisiva. [5] All these cases were caused by TT and had underlying systemic or local immunosuppression. These reports indicate that immunosuppression may perhaps play an important role in the development of the unique clinical features mimicking TI. Narang et al. [6] have also reported a case of T. capitis with underlying systemic immunosuppression (human immunodeficiency virus positive); due to TT presenting with concentric rings. Lim and Smith [7] have described extensive T. corporis caused by TT, resembling TI in a 14-year-old girl; recipient of renal transplant on immunosuppressive therapy.
Batta et al. [8] have also documented two cases of T. corporis due to TT and TM which mimicked TI; they were on cyclical therapy with topical steroid and antifungal. They postulated that prolonged therapy with topical antifungals and corticosteroids may produce lesions that resemble morphologically TI; due to underlying immunosuppression with topical corticosteroids and reinfection due to early discontinuation of topical antifungals. Lee et al. [9] and Sun and Ho [10] have reported T. corporis mimicking TI caused by Microsporum ferrugineum and Microsporum gypseum respectively [Table - 1].
To conclude, it may be stated that both immuno competent and immunosuppressive patients with T. corporis of all ages may present morphologically with concentric rings similar to TI irrespective of the etiological species.
| 1. |
Rippon JW. The pathogenic fungi and pathogenic actinomycetes. Medical Mycology. 2 nd ed. Philadelphia: WB Saunders Co; 1982. p. 154-87.
[Google Scholar]
|
| 2. |
Hryncewicz-Gwó´zd´z A, Beck-Jendroschek V, Brasch J, Kalinowska K, Jagielski T. Tinea capitis and tinea corporis with a severe inflammatory response due to Trichophyton tonsurans. Acta Derm Venereol 2011;91:708-10.
[Google Scholar]
|
| 3. |
Chandra RK. Nutrition and the immune system: an introduction. Am J Clin Nutr 1977;66:4605-35.
[Google Scholar]
|
| 4. |
Chandra RK. Cell-mediated immunity in nutritional imbalance.J Fed Proc 1980;39:3088-92.
[Google Scholar]
|
| 5. |
Ouchi T, Nagao K, Hata Y, Otuka T, Inazumi T. Trichophyton tonsurans infection manifesting as multiple concentric annular erythemas. J Dermatol 2005;32:565-8.
[Google Scholar]
|
| 6. |
Narang K, Pahwa M, Ramesh V. Tinea capitis in the form of concentric rings in an HIV positive adult on antiretroviral treatment. Indian J Dermatol 2012;57:288-90.
[Google Scholar]
|
| 7. |
Lim SP, Smith AG. Tinea pseudoimbricata: Tinea corporis in a renal transplant recipient mimicking the concentric rings of tinea imbricata. Clin Exp Dermatol 2003;28:331-4
[Google Scholar]
|
| 8. |
Batta K, Ramlogan D, Smith AG, Garrido MC, Moss C. Tinea indecisiva may mimic the concentric rings of tinea imbricata. Br J Dermatol 2002;147:384.
[Google Scholar]
|
| 9. |
Lee KH, Lee ES, Kang WH, Lee S. An unusual clinical manifestation of tinea corporis caused by Microsporon ferrugenium. Korean J Dermatol 1987;25:383-8.
[Google Scholar]
|
| 10. |
Sun PL, Ho HT. Concentric rings: An unusual presentation of tinea corporis caused by Microsporum gypseum. Mycoses 2006;49:150-1.
[Google Scholar]
|
Fulltext Views
3,055
PDF downloads
1,587





![[Figure - 1]](#fig_ijdvl_2013_79_4_554_113109_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_4_554_113109_f2.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2013_79_4_554_113109_t3.jpg){kind=link}