Translate this page into:
Unilateral Beau's lines in a case of complex regional pain syndrome (reflex sympathetic dystrophy)
2 Department of Neurology, Ankara Numune Education and Research Hospital, Neurology Clinic, Ankara, Turkey
3 Department of Physical Medicine and Rehabilitation, Ankara Numune Education and Research Hospital, Ankara, Turkey
Correspondence Address:
M�zeyyen G�n�l
Ankara Numune Education and Research Hospital, Dermatology Clinic, Yildizevler Mah. 742.Sok, A Blok No: 3/3 �ankaya/Ankara
Turkey
| How to cite this article: G�n�l M, �akmak SK, Yayla D, Oguz ID, Mungan S, Sivas F. Unilateral Beau's lines in a case of complex regional pain syndrome (reflex sympathetic dystrophy). Indian J Dermatol Venereol Leprol 2012;78:775 |
Sir,
Complex regional pain syndrome (CRPS) type 1 or reflex sympathetic dystrophy (RSD) is a highly painful, poorly understood syndrome, which arises usually after trauma and exceeds in both magnitude and duration of the expected clinical course of the triggering event. [1],[2],[3]
Although RSD has various cutaneous symptoms, it is a rarely seen disorder in dermatology clinics. [2] Some nail findings have been reported in patients with RSD. [4] We present the second case of RSD associated with unilateral Beau′s line.
A 34-year-old woman attended with persistent pain, hyperhidrosis, and edema of right hand, which had been present for 2 years. She denied any initiating event. Her past medical history was nonsignificant. Physical examination revealed significant purple-red erythema, edema, and coldness on her right hand, and it was quite sensitive with touch when both hands were compared [Figure - 1]. Right palm was moist and iodine-starch powder test was positive [Figure - 2]. Beau′s lines were observed on the nails of the right hand [Figure - 3]. Peripheral pulses were positive. Adson test was negative. Her neurologic examination was normal except hyperalgesia, and her visual analog score was 8. Tinnel and Phalen signs were negative.
 |
| Figure 1: Erythematous, edematous, and moist appearance of the right hand |
 |
| Figure 2: Positive iodine-starch powder test |
 |
| Figure 3: Beau's lines on the nails of the right hand, small picture: Close appearance of Beau's lines |
Laboratory tests including erythrocyte sedimentation rate (ESR), C-reactive protein, complete blood count, thyroid function tests, and serum auto-antibodies [antinuclear antibody (ANA), anti-thyroid antibodies, Venereal Disease Research Laboratory (VDRL) test, Extractable Nuclear Antigen Antibodies] produced normal results. X-rays of cervical and upper extremities were normal. Magnetic resonance imaging (MRI) of right hand showed severe edema of the soft tissue [Figure - 4]. Three-phase bone scanning showed increased radionucleotide accumulation in soft tissue of metacarpal region; the bones were normal. The patient was diagnosed as RSD with clinical findings and radiographic tests. Gabapentin therapy (900 mg/d) was suggested. Efficiency of this treatment is unknown because she did not come for follow-up.
 |
| Figure 4: Soft tissue edema of right hand and increased amount of fluid in scaphoid-trapezoid joint space and 4th metacarpophalangeal joint space on the MRI |
RSD is an uncommon disease. Carcinomas, infections, trauma, iatrogenic, ischemic, neurologic, and arthritic events may give rise to RSD. [4] In 10-26% patients with RSD, no inciting factor can be found as in our case. [5]
There are various concepts to explain the etiopathogenesis of RSD. It is thought that RSD is an inflammatory process. Inflammatory mediators, including tumor necrosis factor (TNF)-α, interleukin-1, 2, 6, were shown to be elevated in the blister fluid. [1],[5] The other pathophysiologic mechanisms were alterations in cutaneous innervation, central and peripheral sensitization, altered function of the sympathetic nervous system, lower systemic levels of anti-inflammatory cytokines, genetic factors, autoimmunity, and psychological factors. [1],[3],[5]
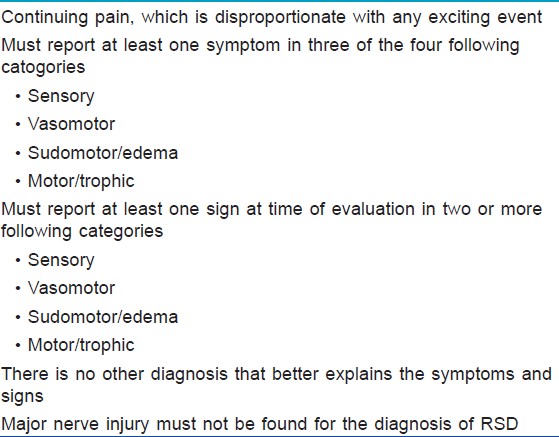
The diagnosis of the disease is clinical; the diagnostic Budapest Criteria are widely accepted [Table - 1]. [1] The ESR, C-reactive protein, complete blood count, and serum auto-antibodies results are useful in ruling out infections and rheumatologic conditions. MRI is often necessary to rule out bone or soft tissue pathology as the source of pain. Three-phase bone scanning of the affected extremity may detect osseous changes. [5] Our case fulfilled Budapest Criteria. Clinical findings and results of MRI and bone scanning were consistent with second stage of RSD.
RSD has been divided into three stages of progression, but it is not necessary for each patient to develop all stages: Acute stage is characterized by burning pain and sensory abnormalities, signs of vasomotor dysfunction and sudomotor disturbance, dystrophic stage is characterized by more marked pain/sensory dysfunction, and atrophic stage is characterized by markedly increased motor/trophic changes. [3],[4],[5] Skin findings of RSD include swelling, color changes, hyperhydrosis, hypohydrosis, hypertrichosis, hypotrichosis, scaling, bullae, erosions, ulcerations, petechiae, telangiectasia, pallor, and atrophy on the affected limb. [1],[3] Nail findings such as leukonychia, nailfold swelling, clubbing, trachyonychia, and Beau′s lines have been reported rarely. [4] Our case is the second case of RSD associated with Beau′s lines in the literature.
Beau′s lines are transverse linear depressions in the nail plate and they occur with transient decrease in the nail plate production at the same localization of the nail plate in most or all of the nails. They may be seen in infectious diseases, renal failure, febrile illnesses, pustular psoriasis, Stevens-Johnson syndrome, drug therapies, and traumatic disorders of extremities. [4] The authors presented four potential explanations for Beau′s lines associated with RSD in the previous case; the physical event precipitating RSD, the relative inactivity of the limb, the matrix being pressed down by edema of hand, and sympathetic denervation might have triggered the development of Beau′s lines. [4] Those might be the pathogenetic mechanisms; in addition to these, we think that inflammatory cytokines such as TNF-α, interleukin-1, 2, 6 that were shown to be increased in RSD might have caused Beau′s lines.
| 1. |
Goebel A. Complex regional pain syndrome in adults. Rheumatology (Oxford) 2011;50:1739-50.
[Google Scholar]
|
| 2. |
Araki E, Tanioka M, Miyachi Y, Utani A. A case of complex regional pain syndrome: An underdiagnosed condition in dermatology. Acta Derm Venereol 2007;87:440-1.
[Google Scholar]
|
| 3. |
Phelps GR, Wilentz S. Reflex sympathetic dystrophy. Int J Dermatol 2000;39:481-6.
[Google Scholar]
|
| 4. |
O'Toole EA, Gormally S, Drumm B, Monaghan H, Watson R. Unilateral Beau's lines in childhood reflex sympathetic dystrophy. Pediatr Dermatol 1995;12:245-7.
[Google Scholar]
|
| 5. |
Sebastin SJ. Complex regional pain syndrome. Indian J Plast Surg 2011;44:298-307.
[Google Scholar]
|
Fulltext Views
3,551
PDF downloads
3,356





![[Figure - 1]](#fig_ijdvl_2012_78_6_775_102397_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_6_775_102397_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_6_775_102397_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2012_78_6_775_102397_f4.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2012_78_6_775_102397_t5.jpg){kind=link}