Translate this page into:
Unilateral Blaschkoid Darier's disease over the forehead
Correspondence Address:
Ashok Krishnarao Ghorpade
BK D-18, Sector 9, Bhilai - 490 006, Chhattisgarh
India
| How to cite this article: Ghorpade AK. Unilateral Blaschkoid Darier's disease over the forehead. Indian J Dermatol Venereol Leprol 2014;80:189-190 |
Sir,
A 73-year-old woman presented with a 6-year history of asymptomatic, greasy, warty, brownish skin lesions over the right side of forehead. Her lesions were worse in the summer and after sun exposure. No other family member had a similar illness. Cutaneous examination showed multiple dark brown, greasy, warty, flat topped papules 2-8 mm in size, with adherent crusts and scales in a linear band on right side of forehead extending inside the scalp in a segmental fashion [Figure - 1]. There were no other skin/mucosal lesions, nail changes, or systemic complaints. Biopsy from the scaly papules showed hyperkeratosis, parakeratosis, follicular plugging, intraepidermal suprabasal cleft with several acantholytic cells and dyskeratosis (in the form of corps ronds and grains) in the epidermis, while the dermis showed a mild chronic inflammatory dermal infiltrate [Figure - 2].
 |
| Figure 1: Greasy, warty, flat-topped brownish papules with adherent crusts and scales in a linear band on right side of forehead extending into the scalp |
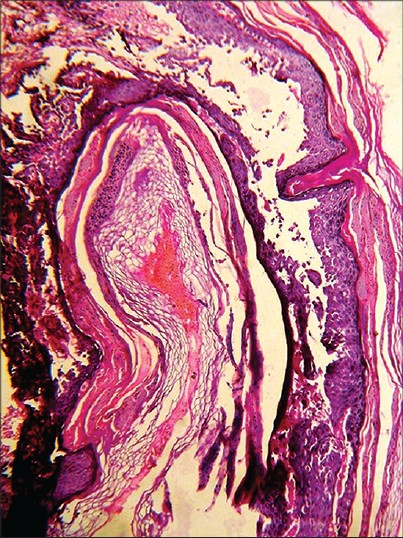 |
| Figure 2: Hyperkeratosis, parakeratosis, follicular plugging, suprabasal cleft with acantholytic cells, and dyskeratoses with corps ronds in spinous layer and grains in stratum corneum (H and E, original magnification, ×100) |
Darier′s disease is an autosomal dominant genodermatosis characterized by symmetrically distributed, greasy, warty papules in a seborrheic distribution on the face and trunk observed mostly in adult patients. Exposure to sunlight and moist hot weather worsen disease. Pitting or punctuate keratoses may be present on the palms and soles. The nails are fragile, splintered with distal triangular nicking, with subungual hyperkeratosis and white and red alternating longitudinal bands. [1] An uncommon linear variant of this condition was first reported in 1906, which lacks the classical features of Darier disease, and only shows localized lesions in a linear fashion. Usually there is no family history. [2],[3],[4],[5],[6] Two subtypes are described, type 1 is commoner, presents along the lines of Blaschko, and is suggested to result from postzygotic somatic mutations. Type 2 is rarer, more severe, characterized by linear streaks and results from a heterozygous germline mutation including somatic loss of heterozygosity of the wildtype allele in a segmental area. [2],[3],[4]
Starink and Woerdeman [3] suggested the term "acantholytic dyskeratotic epidermal nevus", while describing seven cases showing unilateral, linear, or zosteriform patterns. Boente Mdel et al., [4] reported severe localized type 2 variety of linear Darier disease in two siblings blaming loss of heterozygosity for the Darier′s disease gene, located at chromosome 12,12q23-24.1 thereby causing faulty organization of the tonofilaments. Its association with palmoplantar papules and nail disorders has also been described. [5] Gilaberte et al., [6] reported three cases of subtype 1 of localized Darier disease. Some consider this variant a localized form of Darier′s disease, while others believe that it is a variant of epidermal nevus. Inflammatory linear verrucous epidermal nevus (ILVEN), linear psoriasis, linear lichen planus, linear Hailey-Hailey disease and verrucous epidermal nevi, eczema, dermatitis herpetiformis, and Grover′s disease may be considered in the differential diagnosis, but histopathology is confirmatory. Though localized Darier disease has been described earlier, localization of lesions to the scalp has been reported only once earlier in a women and her daughter. [2]
In the present patient, the absence of skin lesions in her family, the localized linear distribution of skin lesions, and characteristic histopathological changes confirmed the diagnosis. She responded well to topical tretinoin cream 0.05% and sunscreens, resulting in significant regression of skin lesions in 4 months. There was recurrence of a few lesions in the next summer which responded to the same treatment. The late age of onset, involvement of forehead extending into the scalp and presence of crusted plaques were unusual features in our case.
| 1. |
O'Malley MP, Haake A, Goldsmith L, Berg D. Localized Darier disease. Implications for genetic studies. Arch Dermatol 1998;133:1134-8.
[Google Scholar]
|
| 2. |
Wheeland RG, Donaldson ML, Bulmer GS. Localized Darier's disease of the scalp complicated by Trichophyton tonsurans infection. Arch Dermatol 1985;121:905-7.
[Google Scholar]
|
| 3. |
Starink TM, Woerdeman MJ. Unilateral systematized keratosis follicularis: A variant of Darier's disease or an epidermal naevus (acantholytic dyskeratotic epidermal naevus)? Br J Dermatol 1981;105:207-14.
[Google Scholar]
|
| 4. |
Boente Mdel C, Frontini Mdel V, Primc NB, Asial RA. Linear Darier disease in two siblings. An example of loss of heterozygosity. Ann Dermatol Venereol 2004;131:805-9.
[Google Scholar]
|
| 5. |
Munro CS, Cox NH. An acantholytic dyskeratotic epidermal naevus with other features of Darier's disease on the same side of the body. Br J Dermatol 1992;127:168-71.
[Google Scholar]
|
| 6. |
Gilaberte M, Puig L, Vidal D, Alomar A Acantholytic dyskeratotic naevi following Blaschko's lines: A mosaic form of Darier's disease. J Eur Acad Dermatol Venereol 2003;17:196-9.
[Google Scholar]
|
Fulltext Views
3,465
PDF downloads
2,200





![[Figure - 1]](#fig_ijdvl_2014_80_2_189_129423_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_2_189_129423_f2.jpg){kind=link}