Translate this page into:
Unilateral distribution of cutaneous metastasis in a case of colon carcinoma
2 Department of Pathology, University Hospital of Marqués de Valdecilla, Cantabria, Santander, Spain
Correspondence Address:
Carlos Duran Vian
Hospital Universitario Marqués de Valdecilla, Av. Valdecilla, 25, 39008 Santander, Cantabria
Spain
| How to cite this article: Duran Vian C, Vilanova-Urdániz I, Pérez Paredes G, González-Vela M C, González-López MA. Unilateral distribution of cutaneous metastasis in a case of colon carcinoma. Indian J Dermatol Venereol Leprol 2019;85:93-96 |
Sir,
Cutaneous metastasis from primary internal malignancies represent 0.7–9% of metastasis in patients with cancer.[1] Clinically, cutaneous metastasis usually appears as painless nodules. However, a wide spectrum of clinical presentations have been described: inflammatory erysipelas-like lesions, diffuse sclerodermiform lesions with induration, telangiectatic papulovesicles, purpuric plaques mimicking vasculitis, alopecia areata-like scalp lesions and lesions in a zosteriform pattern.[2] Frequency of skin metastasis of colon tumors has been reported to be 2.3–6% in cases of metastatic colorectal cancer. They usually develop within 2 years after the resection of the primary tumor. The most common site of colon cancer metastasis is the abdominal skin, often on surgical scars.[3],[4] In the umbilical region, they are known as Sister Mary Joseph's nodule. Here, we describe an unusual case of cutaneous metastases of colorectal carcinoma with extensive predominantly unilateral distribution.
A 71-year-old woman was diagnosed 3 months ago with a left-sided colon adenocarcinoma stage IV with adrenal and ganglionic left side metastasis. Trousseau's syndrome and endometrial cancer were also diagnosed. The patient was under palliative chemotherapy with oxaliplatin and capecitabine. After the fifth cycle of chemotherapy, she developed multiple asymptomatic cutaneous lesions on the upper left limb and the left hemi-thorax, which progressively spread to the lower limb. Dermatological examination revealed multiple erythematous purplish, infiltrated plaques unilaterally distributed on the left side of her body with marked edema on both upper and lower left limbs. These cutaneous lesions had a tendency to respect the midline almost in its entirety [Figure - 1]. Blood analysis showed normocytic normochromic anemia and slight eosinophilia. A computerized axial tomography showed prominent left clavicle and abdomino-pelvic lymphadenopathy, as well as multiple venous thrombi mostly located in the left jugular internal vein and left subclavian vein confluence.
 |
| Figure 1 |
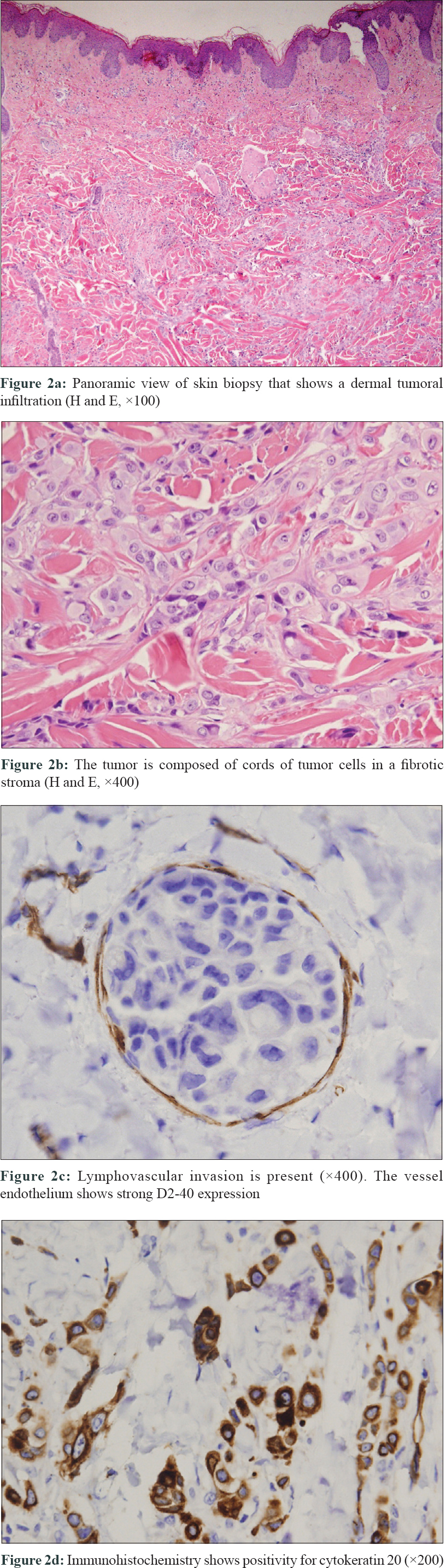
A biopsy of the skin lesions was performed. Histopathologic examination showed an extensive infiltration of the dermis by tumor cells dispersed in a dense fibrous stroma. [Figure - 2]a. The tumor was composed of cords of tumor cells and focal ductal differentiation [Figure - 2]b. There was vascular invasion of the superficial dermal lymphatics [Figure - 2]c. Immunostaining revealed that the tumor cells were positive for cytokeratin 20 [Figure - 2]d and epithelial membrane antigen (EMA) but negative for cytokeratin 7, estrogen receptors and paired box gene 8 (PAX8). These histopathological and immunohistochemical findings were consistent with metastatic colonic adenocarcinoma.
 |
| Figure 2 |
Despite chemotherapy, 2 months later, the patient died. The skin lesions and swelling of the limbs had progressed predominantly in left half of the body during this period.
Cases of skin metastasis with extensive unilateral distribution are extremely rare. We only found a single case of disseminated melanoma with a similar distribution reported in the literature.[5] It is difficult to explain the reason why the skin metastatic lesions developed unilaterally in our patient. Nevertheless, it is possible that the previous venous thrombosis might have influenced the occurrence of this peculiar clinical presentation. To this end, it should be noted that the thoracic duct collects most of the lymph of the body except from the right thorax, arm, head and neck, which are drained by the right lymphatic duct. The thoracic duct drains into the systemic circulation at the confluence of the left internal jugular vein and left subclavian vein, coincidentally where our patient had large and recurrent thrombi (Trousseau's syndrome), as the computerized axial tomography scan showed. Considering that the spread occurred through lymphatics, this induced slowdown of lymph flow could explain, at least in part, the presence of left-sided cutaneous metastasis. However, no postmortem examination was obtained to support this hypothesis.
In summary, the case presented here highlights the relevance of including cutaneous metastases in the differential diagnosis of patients with multiple cutaneous lesions with unilateral patterns of distribution, contemplating the possibility of associated thrombosis, especially in those with an underlying neoplasm recently diagnosed.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Lookingbill DP, Spangler N, Helm KF. Cutaneous metastases in patients with metastatic carcinoma: A retrospective study of 4020 patients. J Am Acad Dermatol 1993;29:228-36.
[Google Scholar]
|
| 2. |
Lookingbill DP, Spangler N, Sexton FM. Skin involvement as the presenting sign of internal carcinoma. A retrospective study of 7316 cancer patients. J Am Acad Dermatol 1990;22:19-26.
[Google Scholar]
|
| 3. |
Nesseris I, Tsamakis C, Gregoriou S, Ditsos I, Christofidou E, Rigopoulos D. Cutaneous metastasis of colon adenocarcinoma: Case report and review of the literature. An Bras Dermatol 2013;88:56-8.
[Google Scholar]
|
| 4. |
Saeed S, Keehn CA, Morgan MB. Cutaneous metastasis: A clinical, pathological, and immunohistochemical appraisal. J Cutan Pathol 2004;31:419-30.
[Google Scholar]
|
| 5. |
Ariel IM. Disseminated melanoma with unique unilateral distribution. Cancer 1975;36:2143-6.
[Google Scholar]
|
Fulltext Views
3,725
PDF downloads
3,323





![[Figure - 1]](#fig_ijdvl_2019_85_1_93_246744_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2019_85_1_93_246744_f2.jpg){kind=link}