Translate this page into:
Unilateral pruritus following stroke
2 Department of Radiodiagnosis, Pondicherry Institute of Medical Sciences, Puducherry, India
Correspondence Address:
Satyaki Ganguly
Department of Dermatology, Venereology and Leprosy, Pondicherry Institute of Medical Sciences, Pondicherry - 605 014, Puducherry
India
| How to cite this article: Ganguly S, Krishna C V, Parmar NV, Kuruvila S, Phansalkar DS. Unilateral pruritus following stroke. Indian J Dermatol Venereol Leprol 2015;81:186-188 |
Sir,
Post-stroke pruritus is a rare type of central itch resulting from lesions within the brain that affect afferent neural pathways, controlling centres or modulating regions of itch. However, its exact pathophysiology is unclear.
A 52-year-old male presented to the dermatology outpatient department with severe and continuous itching on the left side of his body of 10 days duration. He was on treatment for systemic hypertension for the past 4 years. Three weeks before presentation to us, he had a cerebrovascular accident with left-sided hemiparesis from which he recovered. Cutaneous examination revealed numerous excoriations over the left arm, left side of the trunk, and left thigh with complete sparing of the right side of the body [Figure - 1].
 |
| Figure 1: Numerous excoriations over the left arm, left side of the trunk with complete sparing of the right side |
Haematological and biochemical investigations were normal except for dyslipidaemia. A computed tomography scan done 3 weeks prior to this, showed multiple infarcts involving the left cerebellar hemisphere. Magnetic resonance imaging with magnetic resonance angiography, also performed 3 weeks ago, showed acute infarcts in various areas of the brain [Figure - 2] but mainly involving the distribution of right anterior and middle cerebral arteries. Of note, lacunar infarcts were seen involving the right internal capsule and parts of right thalamus. In addition, the left lobe of cerebellum showed chronic infarcts with surrounding gliosis. Based on this background of unilateral pruritus after a recent stroke and normal renal, liver, and endocrinological function, a diagnosis of post-stroke pruritus was made and the patient started on tablet amitriptyline 25 mg once daily. Follow-up after 15 days revealed marked improvement of pruritus.
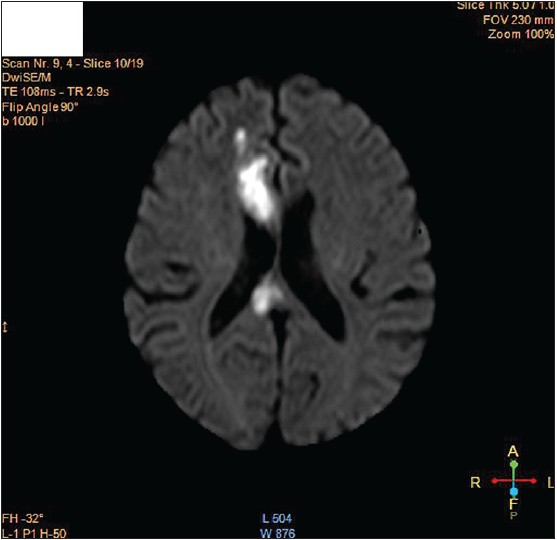 |
| Figure 2: Acute infarcts were seen involving the right frontal lobe, genu and splenium of corpus callosum |
Post-stroke pruritus was first described due to infarction of the internal capsule. [1] It has also been reported after contralateral thalamic stroke and cerebral infarction in the middle cerebral artery distribution. [2] In a case series of nine patients, five had involvement of the thalamus and subcortical regions. [3] Localized pruritus has also been described in many neurological disorders, such as multiple sclerosis, brain tumours, and brain abscess. [2],[3] Post-stroke pain is well known and more frequently documented compared to post-stroke pruritus, although both are mediated by anatomically identical, but functionally distinct C-fibres. [2] Moreover, it has also been found that the brain areas activated during itch and pain have some degree of overlap. Further, pruritus remits with painful stimuli. [4] Another possible evidence in support of the relation between the two entities is the responsiveness of post-stroke pruritus to treatment with amitriptyline, a drug used as a first-line treatment option for central post-stroke pain.
The sensation of itch is multidimensional and involves different areas of the brain, such as anterior cingulate cortex, premotor area, primary somatosensory cortex, insular cortex, supplementary motor area, cerebellum and thalamus. A centre in the medulla is also believed to control scratching. Ischemic strokes involving the lateral medulla preferentially produce facial neuropathic itch that can lead to trigeminal trophic syndrome. The cerebellum might also act as a coordinating centre for the itch-scratch cycle. [5] Our patient had acute infarcts affecting the right frontal lobe, right centrum semiovale, genu and splenium of corpus callosum on the right side. He also had lacunar infarcts in the genu, posterior limb of right internal capsule and right thalamus. This explains the left-sided unilateral pruritus. However, bilateral central pruritus due to a unilateral brain lesion has also been described, though with a unilateral onset or predominance. [4] Onset of this condition is always delayed, but may be episodic lasting from several seconds to minutes, unlike the continuous pruritus in our case. [4]
This report highlights the need for having a high index of suspicion for post-stroke pruritus in patients presenting with unilateral itch in the aftermath of a stroke. A detailed history, complete clinical examination and relevant imaging studies of brain are necessary to establish a diagnosis. Further, accurate analysis of central nervous system findings in patients with unilateral pruritus after stroke could reveal fascinating insights into the ill-defined pathomechanisms of central itch.
| 1. |
King CA, Huff FJ, Jorizzo JL. Unilateral neurogenic pruritus: Paroxysmal itching associated with central nervous system lesions. Ann Intern Med 1982;97:222-3.
[Google Scholar]
|
| 2. |
Kimyai-Asadi A, Nousari HC, Kimyai-Asadi T, Milani F. Poststroke pruritus. Stroke 1999;30:692-3.
[Google Scholar]
|
| 3. |
Massey EW. Unilateral neurogenic pruritus following stroke. Stroke 1984;15:901-3.
[Google Scholar]
|
| 4. |
Canavero S, Bonicalzi V, Massa-Micon B. Central neurogenic pruritus: A literature review.Acta Neurol Belg 1997;97:244-7.
[Google Scholar]
|
| 5. |
Hassan I, Haji ML. Understanding itch: An update on mediators and mechanisms of pruritus. Indian J Dermatol Venereol Leprol 2014;80:106-14.
[Google Scholar]
|
Fulltext Views
12,316
PDF downloads
1,558





![[Figure - 1]](#fig_ijdvl_2015_81_2_186_152294_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_2_186_152294_f2.jpg){kind=link}