Translate this page into:
Unilateral segmental type II leiomyomatosis: A rare occurrence
Correspondence Address:
Resham J Vasani
A/1 Sharad Kunj, Dr. Moose Road, Thane (West) 400602
India
| How to cite this article: Vasani RJ. Unilateral segmental type II leiomyomatosis: A rare occurrence. Indian J Dermatol Venereol Leprol 2012;78:521 |
Sir,
Twenty two years old unmarried male presented with pale red colored lesions in a grouped fashion on the left side of the upper and lower back since past four years. The lesions started initially over the upper back and over a period of one year, appeared over the lower back. The lesions were occasionally mildly painful on pressure. There was no history of cold sensitivity or associated systemic complaints. There was a history of similar lesions in his 60 year old mother on the lower back, the detailed history and examination of whom was not possible since she resided in the village. Siblings were normal.
On examination, there were flesh colored erythematous, firm, dome-shaped papulonodular lesions in an agminate fashion and spanning two separate non-conjoint segments on the upper and lower back on the left side of the body [Figure - 1]a, b. The lesions were minimally tender on firm pressure. An application of ice over the lesions elicited minimal pain and burning sensation. Rest of the cutaneous and systemic examination was normal.
 |
| Figure 1: (a, b) Multiple erythematous papulo nodular lesions distributed in a grouped segmental fashion on the upper and lower back |
A diagnosis of segmental cutaneous leiomyomatosis was made.
All investigations including hemogram, urine analysis, liver and renal function tests, chest X-ray, and ultrasonography of abdomen, computerized tomography of the abdomen and pelvis were normal.
Biopsy showed a tumor, composed of irregularly arranged smooth muscle fibers, with elongated nuclei and rounded ends, interlaced with variable amounts of collagen in the reticular dermis [Figure - 2]a, b. Masson′s trichrome stained the smooth muscles dark red [Figure - 3] confirming the diagnosis of leiomyoma.
Considering the multiplicity of the leiomyomas, the patient was counseled regarding the condition and was started on C. Nifedipine 10 mg thrice daily, which was well-tolerated by the patient with decrease in the symptomatology. He was advised to follow-up for yearly abdominal CT scans, screening of blood relatives and screening of related females for uterine leiomyomas, genetic counseling and testing.
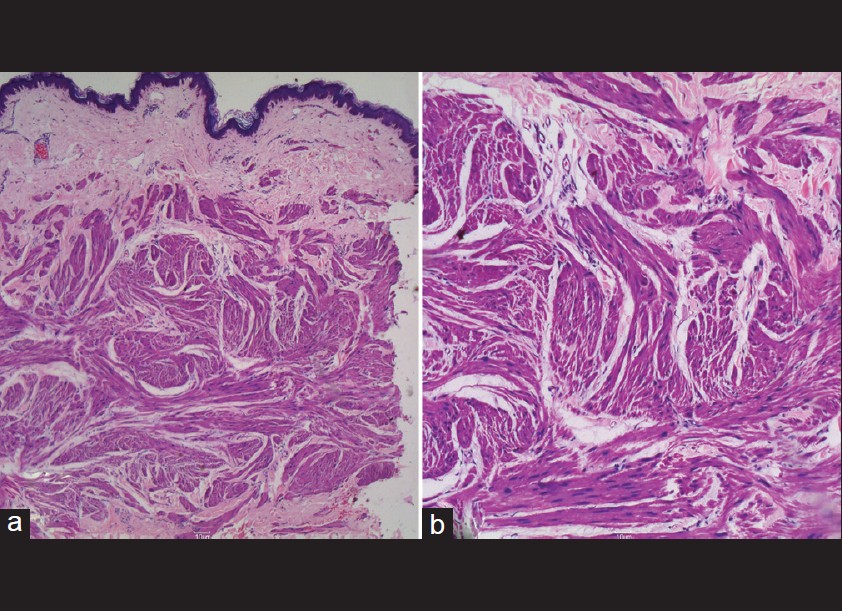 |
| Figure 2: (a) H and E, ×4 - Dermis shows tumor composed of irregularly arranged smooth-muscle fibers, interlaced with variable amounts of collagen in the reticular dermis. (b) H and E, ×40 - Tumor composed of Smooth muscle cells with elongated nuclei and rounded ends |
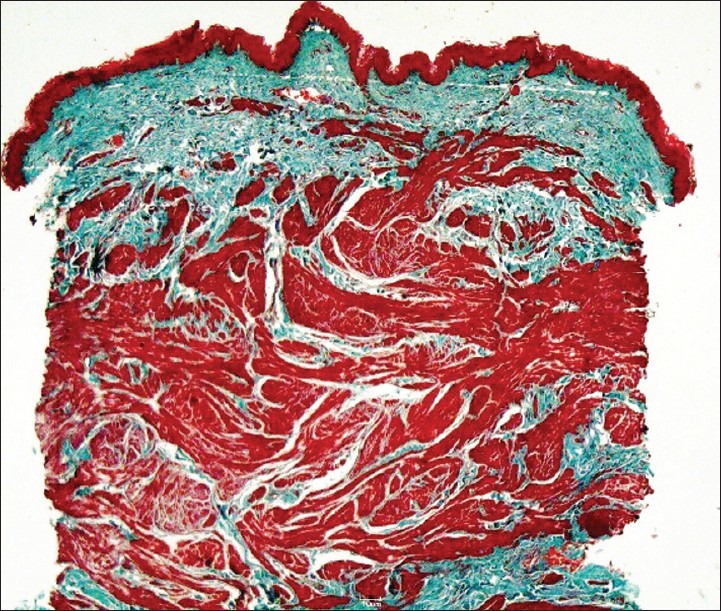 |
| Figure 3: 4X, Masson Trichrome Stain-Smooth muscle tumor stained Dark Red |
Multiple cutaneous and uterine leiomyomas (MCUL) was first described by Reed in 1973. [1] It was found to be an autosomal dominant condition, characterized by the presence of multiple cutaneous leiomyomas, which are benign painful tumors arising from arrector pili muscle and in women of uterine leiomyomas. In a few families, this syndrome predisposes to aggressive kidney cancer, either type II papillary or collecting duct morphology and hence the other name - Hereditary Leiomyomas and Renal cell carcinoma (HLRCC). In these families, there is fumarate hydratase gene heterozygote loss of function mutation at chromosome 1q42.1.
The leiomyomas are sensitive to touch, cold, emotional stress or can be spontaneously painful. The pain can be paroxysmal with burning, pinching or stabbing quality. The most likely causes for the pain are presence of direct impingement of the tumor on the cutaneous nerves. [2] In this case, relatively less painful nature of the leiomyomas was possibly due to absence of such impingement. Other causes cited are infiltration of mast cells, muscle contraction, local vasoconstriction leading to muscle contraction.
On the extremities, leiomyomas are usually solitary, while on the trunk, the lesions are usually multiple and can be disseminated, zosteriform or segmental. Happle proposed 2 theories for segmental leiomyomas. Type I segmental leiomyomas reflects heterozygosity of post zygotic mutation, leading to segmental skin lesions comparable with non-mosaic phenotype. Type II segmental leiomyomatosis reflects post zygotic mutational event in a heterozygous embryo with subsequent loss of heterozygosity, resulting in pronounced pattern of segmental lesions superimposed on ordinary phenotype of underlying disease. [3]
In this case, the patient had leiomyomas, distributed in 2 distinct segments unilaterally on the left side of his body. It was labeled as a type II presentation because the lesions, presented early in life, had the possibility of developing non-segmental lesions later in life, and the mother also had cutaneous leiomyomas possibly in a non-segmental distribution. This presentation is comparable to the case reported by Parmentier et al. [4] wherein they found multiple leiomyomas distributed according to segmental type II distribution, covering several areas exclusively on the left side of the body. Heterozygosity for a mutation c.695delG, leading to a truncated protein p.Gly232AspfsX24, was found to be responsible in their case. Due to constraints, a mutation analysis was not possible in this case. In case of multiple leiomyomas where an excision is impractical, carbon dioxide laser ablation, liquid nitrogen cryotherapy and electrocoagulation has been tried though the chances of recurrence are about 50%. Excision with skin grafting or surgical resection and immediate reconstruction with artificial dermal template can be tried. In most cases, target is pain relief, and other than oral nifedipine, alpha adrenergic blockers like phenoxybenzamine and doxazosin, nitrates, antidepressants, gabapentin have been tried. Oral pulsed hyoscine butyl bromide tablets [5] and intralesional botulinum toxin have been tried.
| 1. |
Garcia MP, Pujol RM, Alomar A. Familial leiomyomatosis cutis et uteri (Reed's syndrome). Arch Dermatol Res 1988; 280:29-32.
[Google Scholar]
|
| 2. |
Mann PR. Leiomyoma cutis - An electron microscopic study. Br J Dermatol 1970; 82:463-9.
[Google Scholar]
|
| 3. |
Thompson JA. Therapy for painful cutaneous leiomyomas. J Am Acad Dermatol 1985; 13:865-7.
[Google Scholar]
|
| 4. |
Parmentier L, Tomlinson I, Happle R, Borradori L. Evidence for a new fumarate hydratase gene mutation in unilateral Type 2 segmental Leiomyomatosis. Dermatology 2010; 221:149-53.
[Google Scholar]
|
| 5. |
Kaliyadan F, Manoj J, Dharmaratnam AD. Multiple cutaneous Leiomyomas: Pain relief with Pulsed Hyoscine Butyl Bromide. Indian J Dermatol 2009; 54:72-4.
[Google Scholar]
|
Fulltext Views
2,414
PDF downloads
1,829





![[Figure - 1]](#fig_ijdvl_2012_78_4_521_98103_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_4_521_98103_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_4_521_98103_u3.jpg){kind=link}