Translate this page into:
Valacyclovir-induced urticaria without acyclovir hypersensitivity
Correspondence Address:
Satyendra K Singh
Department of Dermatology and Venereology, IMS, BHU, Varanasi - 221 005, Uttar Pradesh
India
| How to cite this article: Singh SK, Prabhu A, Kumar A. Valacyclovir-induced urticaria without acyclovir hypersensitivity. Indian J Dermatol Venereol Leprol 2015;81:611-612 |
Sir,
A 40-year-old male presented to the dermatology outpatient department (OPD), S. S. Hospital, Institute of Medical Sciences, BHU, with malaise, generalized pruritus, and urticarial lesions within 6 h of taking two 1000 mg tablets of valacyclovir for a recurrence of herpes labialis. He reported having recurrent episodes of herpes labialis for 8 years, with 2–3 episodes per year. Prior treatment included acyclovir 400 mg 5 times a day for 5 days during the prodromal phase, with reports of resolution within 4-5 days, even if vesiculation occurred.
One day prior to the current episode, the patient experienced burning and itching sensation on the right side of the lower lip, and took 2000 mg valacyclovir orally. Within 5 h of taking valacyclovir, he developed malaise and generalized pruritus and within the next hour, developed multiple, generalized, erythematous and raised lesions. There was no difficulty in breathing. There was no history of any other drug intake or any drug hypersensitivity.
On examination, the temp erature was 98.8°F, pulse rate 82/min, and blood pressure 138/86 mmHg. Muco-cutaneous examination revealed small, grouped vesicles on the right half of lower lip. Multiple erythematous, blanchable plaques varying from 1 × 1 to 3 × 5 cm were scattered over the neck, trunk, and limbs. A complete blood count, liver function tests, and renal function tests revealed a total leukocyte count of 12300/µL and SGOT/SGPT of 56/60 IU/L; the remainder of the parameters were within normal limits. Based on the history and physical examination, a diagnosis of recurrent herpes labialis with valacyclovir-induced urticaria was made.
Valacyclovir was discontinued. A single dose of 40 mg prednisolone along with daily fexofenadine 180 mg was prescribed. The urticarial lesions resolved within 5 h of taking prednisolone. Within a week, the labial lesions healed and no recurrence of pruritus or urticaria was noted.
Two months later, the patient again developed prodromal symptoms and signs of herpes labialis. He took oral acyclovir 400 mg 5 times a day for 5 days, after having prepared for emergency resuscitation if needed. No adverse drug reaction was noted this time.
After approximately 4 months, a new episode of herpes labialis occurred. The patient intentionally took two tablets of valacyclovir, 1000 mg orally to confirm whether he was allergic to valacyclovir, after making sure he was equipped for emergency resuscitation. Within 30 min of oral intake of valacyclovir, he developed itching and myalgia. Within 1 h he developed urticarial lesions all over the body. A single dose of prednisolone 40 mg and fexofenadine, 180 mg was given and he improved symptomatically within 2 h. Fexofenadine 180 mg daily was continued for 4 days and the subsequent dose of valacyclovir was omitted. No signs and symptoms of adverse drug reaction were noted after 5 days.
Most of the drugs have the potential to cause hypersensitivity reactions. Allergic reactions are a well-known adverse effect associated with antibiotics but there is less familiarity with allergic reactions to antiviral medications. Acyclovir has been associated with several types of adverse drug effects, most commonly dermatologic reactions. Dermatitis, pruritus, urticaria, vasculitis, peripheral edema, erythema nodosum and exanthems have been reported after oral acyclovir. Contact dermatitis and macular erythema have occurred following parenteral therapy and topical therapy has resulted in numerous reports of cutaneous reactions.[1],[2],[3],[4] Valacyclovir has also been associated with urticaria, diffuse erythema and pruritus indicative of systemic reactions.[5]
The two antiherpetic agents, acyclovir and valacyclovir, share a common 2-aminopurine nucleus, which may be the part of the molecule responsible for allergenicity [Figure - 1].[5] Because of this structural similarity, valacyclovir is contraindicated in patients with a history of hypersensitivity to acyclovir.[1] We were unable to find any previous report of isolated hypersensitivity to valacyclovir, without acyclovir hypersensitivity.
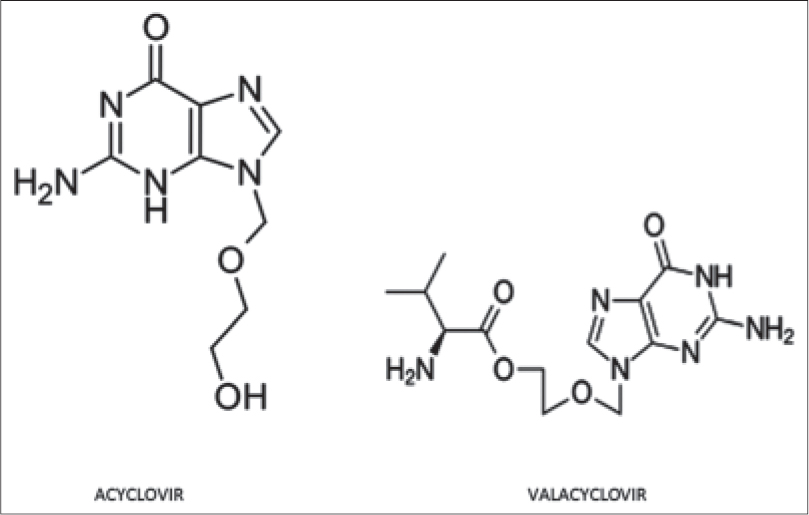 |
| Figure 1: Chemical structure of acyclovir and valacyclovir |
We present a case of recurrent herpes labialis who had taken multiple courses of acyclovir previously, without any adverse events. He developed acute urticaria after taking a single dose of valacyclovir. A trial of acyclovir subsequently did not cause any adverse event, however re-challenge with valacyclovir led to urticaria. This result is difficult to explain because of the structural similarity of these two drugs and similarity of most of the excipients in both formulations. Excipients, which were not common and present in valacyclovir alone, were crospovidone, silica colloidal anhydrous, macrogol, and carnauba wax. We were unable to find any previous reports of hypersensitivity reactions to these excipients. Therefore, the possible explanations include hypersensitivity to the added side chain in valacyclovir or hypersensitivity to the excipients used in valacyclovir.
| 1. |
Carrasco L, Pastor MA, Izquierdo MJ, Fariña MC, Martín L, Fortes J, et al. Drug eruption secondary to aciclovir with recall phenomenon in a dermatome previously affected by herpes zoster. Clin Exp Dermatol 2002;27:132-4.
[Google Scholar]
|
| 2. |
Schuster J, Fabri M, Eming S, Hunzelmann N. Allergic drug eruption secondary to intravenous acyclovir. Acta Derm Venereol 2008;88:196-8.
[Google Scholar]
|
| 3. |
Gola M, Francalanci S, Brusi C, Lombardi P, Sertoli A. Contact sensitization to acyclovir. Contact Dermatitis 1989;20:394-5.
[Google Scholar]
|
| 4. |
Vernassiere C, Barbaud A, Trechot PH, Weber-Muller F, Schmutz JL. Systemic acyclovir reaction subsequent to acyclovir contact allergy: Which systemic antiviral drug should then be used? Contact Dermatitis 2003;49:155-7.
[Google Scholar]
|
| 5. |
Lammintausta K, Makela L, Kalimo K. Rapid systemic valaciclovir reaction subsequent to aciclovir contact allergy. Contact Dermatitis 2001;45:181.
[Google Scholar]
|
Fulltext Views
7,481
PDF downloads
2,001





![[Figure - 1]](#fig_ijdvl_2015_81_6_611_168346_f1.jpg){kind=link}