Translate this page into:
Zinc responsive acrodermatitis in nephrotic syndrome: A rare presentation
Correspondence Address:
Chitra S Nayak
OPD - 14, Skin and V.D. Department, 2nd floor OPD building, T.N.M.C and B.Y.L Nair Ch. Hospital, Mumbai Central, Mumbai - 400 008, Maharashtra
India
| How to cite this article: Topal AA, Dhurat RS, Nayak CS. Zinc responsive acrodermatitis in nephrotic syndrome: A rare presentation. Indian J Dermatol Venereol Leprol 2012;78:122-123 |
Sir,
A 20 year old male presented with dark colored, itchy, scaly lesions over extremities, buttocks and groin, on and off since 5 years. In the past he had consulted various dermatologists, been diagnosed variably as dermatophytosis/ psoriasis and treated unsuccessfully with topical corticosteroids and oral antifungal agents. He had received diuretics and systemic steroids for idiopathic nephrotic syndrome (NS), diagnosed at the age of 2 years and was on cyclosporine since the last 4 years for the same. There was no history of diarrhoea, decreased appetite, hair loss, repeated infections, alcohol abuse or gastrointestinal surgery. General examination revealed cushingoid features. On cutaneous examination, there were well demarcated, symmetrical, hyperpigmented, scaly plaques over dorsum of feet and hands, groin and perianal region [Figure - 1] and [Figure - 2]. Hair and nails were normal. KOH mount of skin scraping was negative. A differential diagnosis of necrolytic acral erythema and zinc deficiency acrodermatitis were considered.
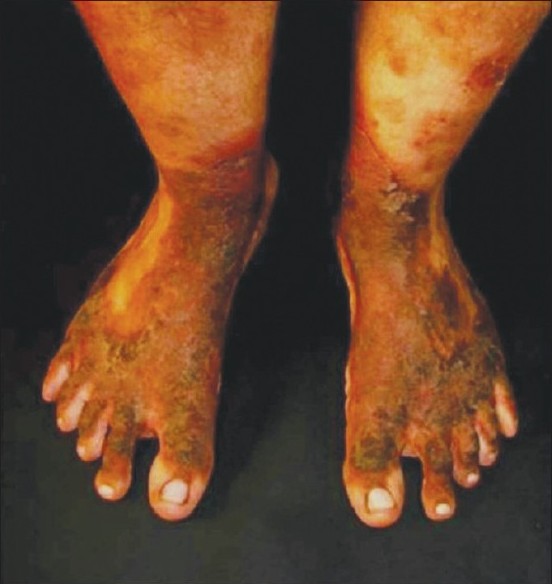 |
| Figure 1: Well demarcated, symmetrical, hyperpigmented, scaly plaques with erythematous rim over dorsum of feet |
 |
| Figure 2: Hyperpigmented scaly plaques over dorsum of hands |
Laboratory investigations revealed hypoproteinemia, hypoalbuminemia and proteinuria with normal renal parameters and negative hepatitis B/ C serology. A lesional biopsy revealed hyperkeratosis, psoriasiform acanthosis, spongiosis, normal granular layer and minimal perivascular mononuclear infiltrate [Figure - 3]. Serum zinc levels: 60 microgram/dl [normal levels: 70-150 microgram/dl] and serum alkaline phosphatase levels: 103 IU (normal levels: >180 IU) clinched the diagnosis of acquired zinc deficiency acrodermatitis due to nephrotic syndrome.
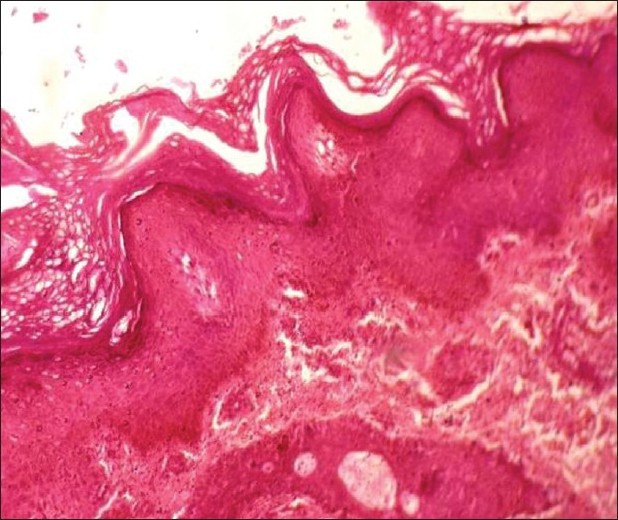 |
| Figure 3: Hyperkeratosis, psoriasiform acanthosis and spongiosis H and E, ×10 |
The patient was started on 1 mg/kg/day of elemental zinc in the form of zinc sulfate 200 mg twice a day (50mg elemental zinc per 220 mg of zinc sulfate) alongwith a topical moisturizer. After one month, there was reduction in scaling, erythema and thickness of plaques with complete clearance over the next 5 months [Figure - 4] and [Figure - 5] at which time, repeat zinc and alkaline phosphatase levels increased to 103 μg/dl and 222 IU respectively. On discontinuing therapy lesions gradually recurred. Repeat zinc level was 66 microgram/dl. Restarting zinc supplementation led to remarkable improvement of lesions.
 |
| Figure 4: Complete clearance of lesions over the feet after zinc therapy |
 |
| Figure 5: Complete clearance of lesions over hands after zinc therapy |
NS patients are reported to be deficient in vitamins B6, B12, A, C, E, D, [1] zinc and copper. [2],[3],[4] It remains unresolved whether low serum zinc concentrations in NS are indicative of true symptomatic or asymptomatic zinc deficiency, or merely reflect a decrease in available zinc-binding proteins, as well over 90% of serum zinc is bound to protein in normal subjects.
The proposed hypotheses for zinc deficiency in NS are:
- loss of intermediate-sized plasma proteins in urine which bind zinc
- concomitant nutritional deficiency
- decreased intestinal absorption
- increased intestinal secretion
Although zinc deficiency has been reported in patients with nephrotic syndrome, the development of cutaneous signs of zinc deficiency in these patients is an uncommon occurrence; an extensive literature search revealing only one such case report. [5] It is unclear why despite low serum zinc levels (mean value: 51.7μg/dl) [3]
in NS, most patients are clinically asymptomatic. Perhaps, concomitant immunosuppression may prevent development of overt skin manifestations or perhaps zinc deficiency in these patients is never severe enough to produce symptoms. However, it is difficult to comment on severity of zinc deficiency based on serum zinc levels alone, since plasma zinc constitutes only 0.1% of total body zinc stores.
In zinc deficiency, an acral and periorificial dermatitis is characteristic, however in chronic zinc deficiency, affection of periorificial areas is rather uncommon. Until now, the exact pathophysiologic mechanisms for many of the skin changes associated with zinc deficiency are unclear.
Zinc is an important component of many metalloenzymes including alkaline phosphatase (ALP) and zinc deficiency leads to decreased serum ALP levels. This may be useful in cases with marginal zinc deficiency with normal serum zinc levels, hence serum ALP level is of crucial importance in suspected zinc deficiency and is recommended. Assays of zinc levels in hair and granulocytes, if available, can be utilized to diagnose marginal zinc deficiency.
Treatment consists of zinc supplementation 0.5-1 mg/kg in divided doses, with higher doses in presence of continuing renal or gastrointestinal loss followed by maintenance dose after clinical resolution. There are no recommended guidelines for duration of therapy and treatment should be tailored for individual patients.
This case is reported due to the rarity of zinc deficiency acrodermatitis in nephrotic syndrome and to emphasize the diagnostic importance of low alkaline phosphatase levels in zinc deficiency.
| 1. |
Podda GM, Lussana F, Moroni G. Abnormalities of homocysteine and B vitamins in the nephrotic syndrome. Thromb Res 2007;120:647-52.
[Google Scholar]
|
| 2. |
Stec J, Podracka L, Pavkovcekova O, Kollar J. Zinc and copper metabolism in nephrotic syndrome. Nephron 1990;56:186-7.
[Google Scholar]
|
| 3. |
Reimold EW. Changes in zinc metabolism during the course of the nephrotic syndrome. Am J Dis Child 1980;134:46-50.
[Google Scholar]
|
| 4. |
Perrone L, Gialanella G, Giordano V, La Manna A, Moro R, Di Toro R. Impaired zinc metabolic status in children affected by idiopathic nephrotic syndrome. Eur J Pediatr 1990;149:438-40.
[Google Scholar]
|
| 5. |
Shah KN, Yan AC. Acquired zinc deficiency acrodermatitis associated with nephrotic syndrome. Pediatr Dermatol 2008;25:56-9.
[Google Scholar]
|
Fulltext Views
4,678
PDF downloads
3,327





![[Figure - 1]](#fig_ijdvl_2012_78_1_122_90976_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_1_122_90976_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_1_122_90976_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2012_78_1_122_90976_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2012_78_1_122_90976_f5.jpg){kind=link}