Translate this page into:
Lichenoid tissue reaction/interface dermatitis: Recognition, classification, etiology, and clinicopathological overtones
2 Skin Institute, School of Dermatology, Greater Kailash, New Delhi, India
3 Department of Pathology, University College of Medical Sciences and Associated Guru Teg Bahadur Hospital, Delhi, India
4 Department of Conservative Dentistry and Endodontics, Government Dental College, Raipur, India
5 Department of Dermatology and STD, University College of Medical Sciences and Associated Guru Teg Bahadur Hospital, Delhi, India
Correspondence Address:
Virendra N Sehgal
Dermato Venerology (Skin/VD) Center, Sehgal Nursing Home, A/6 Panchwati, Delhi 110 033
India
| How to cite this article: Sehgal VN, Srivastava G, Sharma S, Sehgal S, Verma P. Lichenoid tissue reaction/interface dermatitis: Recognition, classification, etiology, and clinicopathological overtones. Indian J Dermatol Venereol Leprol 2011;77:418-430 |
Abstract
Lichenoid tissue reaction or interface dermatitis embrace several clinical conditions, the prototype of which is lichen planus and its variants, drug induced lichenoid dermatitis, special forms of lichenoid dermatitis, lichenoid dermatitis in lupus erythematosus, and miscellaneous disorders showing lichenoid dermatitis, the salient clinical and histological features of which are described to facilitate their diagnosis. Background of lichenoid reaction pattern has been briefly outlined to enlighten those interested in this entity.Introduction
Lichenoid tissue reaction (LTR) or interface dermatitis (IFD) is some of the commonly encountered clinical and histological presentations in dermatology and pathology. The term interface dermatitis refers to the finding in a skin biopsy of an inflammatory infiltrate that abuts or obscures the dermo-epidermal junction. The term ′′lichenoid′′ refers to papular lesion of certain skin disorders of which lichen planus is the prototype. However, this type of reaction can also be seen skin disorders associated with systemic illnesses like lupus erythematosus and the skin changes of potentially fatal disorders such as graft versus host disease, Stevens Johnson syndrome and toxic epidermal necrolysis.
Recognition and Classification
The papules of the prototype lichen planus are shiny, flat-topped, and polygonal, of different sizes and occur in clusters creating a pattern that resembles lichen growing on rock. [1] The reaction can be deduced from the basic feature of epidermal basal cell damage, whether primary or secondary. [2] On histologic examination, the lichenoid lesions are characterized by an infiltrate of inflammatory cells that fills the papillary dermis in a band like fashion and often obscures the dermo-epidermal junction.
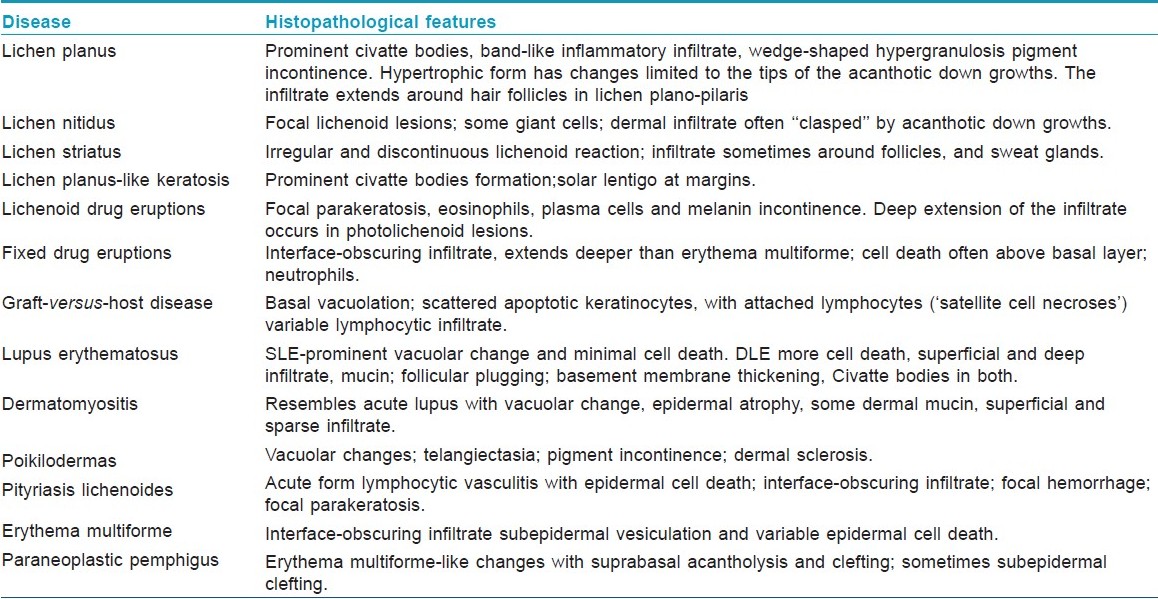
Despite the large spectrum of clinical diseases associated with lichenoid reactions [Table - 1], it can lead to a more meaningful diagnosis through organization of the material in a systematic manner. Historically interface dermatitis has been classified based on predominant cell type in the infiltrate, neutrophilic, lymphocytic or lympho-histiocytic. Some authors also prefer to classify the lymphocytic interface dermatitis by the intensity of the interface inflammation into two broad categories. These include cell poor interface dermatitis when only a sparse infiltrate of inflammatory cells is present along the dermo-epidermal junction, or cell rich where a typically heavy band-like infiltrate is seen which obscures the basal layer of epidermis and is often called lichenoid interface dermatitis. [3] A close cooperation of histopathologist and dermatologist is required to reach confirmatory diagnosis of lichenoid dermatoses.
Etiology
Lichen planus and lupus erythematosus are the most common and best studied representatives of the lichenoid tissue reaction. [4],[5] In lupus erythematosus, basal damage usually is more focal and appears to be secondary, but the events following it are the same. The histologic picture of lichen nitidus is distinctive, but is quite similar to an early lichen planus papule. However, the clinical features of uniform, not enlarging, not confluent round papules, make lichen nitidus a distinctive entity. [6],[7] The lichenoid or lichen planus like actinic keratosis, is another example that basal cell damage, though by a neoplastic process, can lead to a typical lichenoid reaction. [8],[9] Lichenoid drug reactions caused by an ever increasing list of drugs used in medical therapeutics are the commonest culprit in induction of lichenoid dermatitis or lichenoid photodermatitis. [10] Tropical lichen planus or lichen planus actinicus may be sunlight provoked lichen planus or due to direct damage of epidermal basal layer by ultraviolet rays. [11],[12] The current review endeavors to recap the information available thus far in order to facilitate its application in day to day practice.
Dermo--Epidermal Interactions and Pathogenesis
The basal cell damage is a common denominator of these heterogeneous groups of disorders. The term ′′interface dermatitis,′′ often used for lichenoid disorders, denotes that the inflammatory infiltrate along with basal cell damage appear to obscure the dermo--epidermal junction. The epidermal basal cell damage leads to cell death and/or vacuolar changes (liquefactive degeneration). The so-called civatte bodies are damaged epidermal cells with shrunken eosinophilic cytoplasm and pyknotic nuclear remnants (apoptosis), However, certain disorders show frank necrosis of the epidermis rather than apoptosis. Filamentous degeneration is another type of cell damage which, [4] may display none of the above changes. Melanin incontinence is another fall out of the damaged basal cells seen more frequently in drug or solar damage induced dermatoses. [2],[13],[14],[15],[16],[17],[18],[19]
Cell-mediated cytotoxicity is regarded as a major mechanism of pathogenesis of lichen planus, as evidenced by T cells being the predominant cells in the inflammatory infiltrate. [20] Various factors may precipitate the cell mediated reaction resulting in lichen planus lesions such as, mechanical trauma, systemic drugs, contact sensitivity, infective agents including some viruses. [21] Although the specific antigen of LP is still unclear, the antigen presentation by basal keratinocytes are thought to cause T cell accumulation in the superficial lamina propria, basement membrane disruption, intra-epithelial T-cell migration, and CD8+ cytotoxic cell mediated keratinocyte apoptosis in LP. [22]
There is limited data about the role of cell-mediated cytotoxicity in LP, which is mediated by both cytotoxic T lymphocytes (CTL) and natural killer (NK) cells. The cytoplasm of cytotoxic cells is enriched with granules composed of the potent cytolytic molecule perforin (pore-forming protein) together with serine esterase (granzymes). [23],[24] Upon contact with the target cell and activation, CTL and NK cells release perforin and granzymes in a contact zone between target and killer cells. Perforin forms pores in the target cell membrane and thus enables entry of granzymes, responsible for DNA degradation and apoptosis of target cells. Shimizu et al.[25] found a significant role of granzyme B-expressing CD8+ T cells in apoptosis of keratinocytes in lichen planus. Massri et al.,[26] found higher expression of cytolytic molecule perforin in lesional LP as well as in peripheral blood mononuclear cells, as compared to remission and healthy controls, supporting the hypothesis about the potential role of CD8+ cytolytic effector cells in the exacerbation of disease. Similarly, a variety of clinical and pathologic features uniquely observed in FDE lesions can be explained by the presence of CD8+ intraepidermal T cells, with the effector memory phenotype in the FDE lesion. [27],[28]
The possible mechanism involved in the variability of expression of lichenoid tissue reaction depends on the degree and pattern of expression of the intercellular adhesion molecule-1 (ICAM-1). Normal epidermis is resistant to interaction with leukocytes because its keratinocytes have low constitutive expression of ICAM-1. In lichen planus the ICAM-1 expression is limited to the basal keratinocytes while in subacute cutaneous lupus erythematosus, there is a diffuse ICAM-1 expression with basal accentuation. [14],[17] This pattern is induced by ultraviolet (UV) radiation possibly mediated by tumor necrosis factor alpha (TNF-alpha). The histogenesis of lichenoid interface dermatoses is diverse, and includes both cell-mediated and humoral immune responses. [29],[30] Furthermore, recent work has suggested that a number of different LTR/IFD skin disorders share a common inflammatory signaling pathway involving the actions of plasmacytoid dendritic cell-derived interferon-alpha (IFN-alpha). This signaling pathway appears to amplify cytotoxic T cell injury to the epidermal basal cell compartment. The preceding pathway as well as the other cellular and molecular mechanisms that are thought to be responsible for the prototypic LTR/IFD disorder, lichen planus has recently been reviewed. [31]
The subject of lichen planus (LP) and dental metal allergy long has been debated. An overwhelming majority of the existing literature focuses on mercury and gold salts in relation to oral lichen planus. It is an intriguing revelation and subject of investigations. [32] Accordingly, dental materials like mercury and gold and certain drugs may induce epithelial alterations, resembling oral lichen planus (OLP). Although, these alterations do not have all the clinical and/or the histological features of OLP; yet these lesions are known as oral lichenoid lesions (OLLs). Onset and/or worsening of OLLs/OLP after the administration of anti-hepatitis C virus (HCV) therapy have been highlighted. Furthermore, development of symptomatic OLLs, in consequence to anti-HCV therapy (interferon-alpha and ribavirin), in two human immunodeficiency virus-HCV-coinfected subjects has also been described. An immunological cause related to coinfection and administration of different medications too could be responsible for the onset of OLLs. The new reports, together with the previous ones of a possible association between OLP and/or OLLs and anti-HCV therapy, highlight the absolute need to monitor carefully the human immunodeficiency virus-HCV-coinfected subjects who are about to start the anti-HCV therapy and to define better the clinical and histopathological criteria to distinguish OLP from OLLs. [33]
It is intriguing at this point in time, to enlighten that fludarabine, a purine antimetabolite with potent immunosuppressive properties, has previously been associated with the development of transfusion-associated graft versus host disease (TA-GVHD) in patients with hematologic malignancies. Its role as a risk factor for TA-GVHD in patients without underlying leukemia or lymphoma is uncertain.
However, the increasing use of these drugs in the treatment of autoimmune disease might result in occurrence of TA-GVHD after fludarabine therapy. Such an episode-developing in-patient with systemic lupus erythematosus strongly suggests that this drug is sufficiently immunoablative to be an independent risk factor for TA-GVHD. [34] It is therefore, worthwhile to study this aspect in lichenoid interface dermatosis.
Clinicopathological Overtones
Lichen planus and its clinical variants
They are fairly common, extensively covered dermatosis encountered worldwide. The clinical and histological features are well documented. [16],[29],[35],[36],[37] The latter is a classic example of the lichenoid interface dermatitis, and is characterized by the basal cell damage in the form of multiple civatte bodies and a band-like infiltrate on the undersurface of the epidermis along with wedge-shaped hypergranulosis with saw toothed rete-ridges [38] [Figure - 1]. However, individual histopathological variations [Figure - 2] may be seen in the different clinical types of lichen planus [38],[39],[40],[41],[42],[43],[44] and have been excellently recorded by Weedon. [29] Ulcerative lesions are usually seen on mucous membranes of the oral cavity, glans penis and vulva. [45] In such instances, the typical histopathological changes are confined largely to the margins of the ulcer. [46],[47],[48]
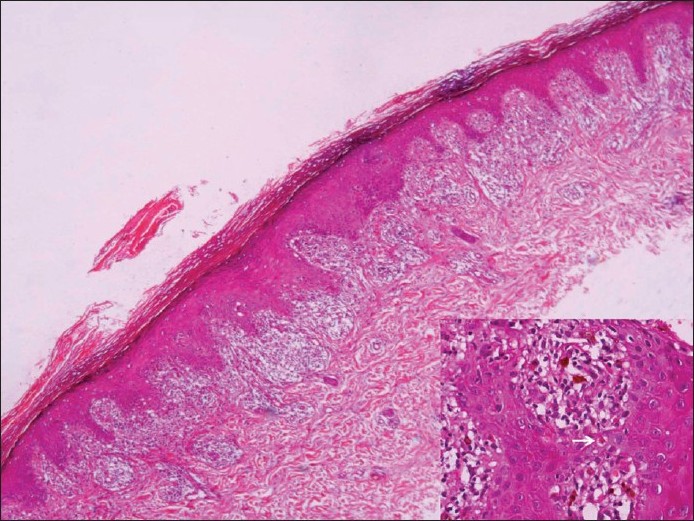 |
| Figure 1: Lichen planus: Section showing hyperkeratosis, hypergranulosis, saw-tooth-like rete and interface dermatitis. High power view showing lichenoid infiltrate and apoptotic keratinocytes (inset, arrow) (H and E, ×40) |
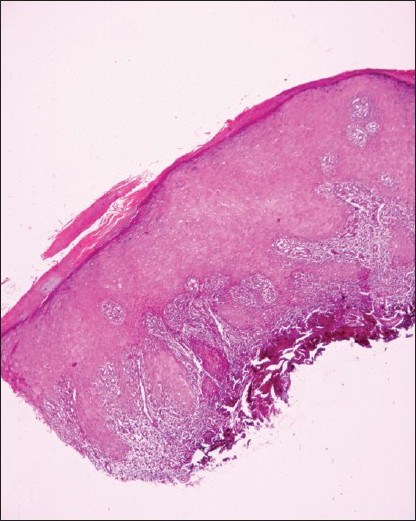 |
| Figure 2: Lichen planus hypertrophicus: Section showing marked hyperkeratosis and epithelial hyperplasia with an otherwise typical band-like infiltrate of lichen planus. (H and E, ×40) |
Lichen nitidus
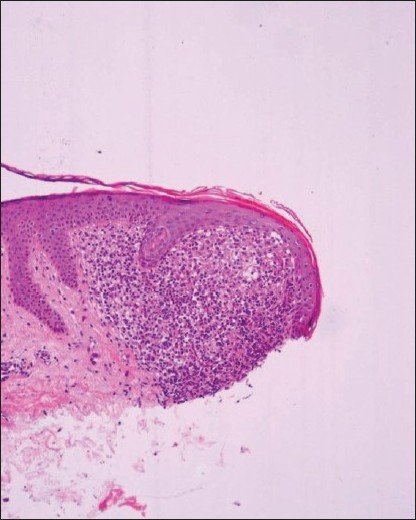
Unlike lichen planus, asymptomatic lesions having predilection for the upper extremities, chest, abdomen, and male genitalia [49],[50],[51],[52],[53] clinically characterize it. Previously recorded summertime actinic lichenoid eruption (SALE), may well represent the actinic form of lichen nitidus. [54] The histopathology is picturesque, a dense, well-circumcised subepidermal infiltrate enclosed by a ′′claw-like′′ rete ridges. [29],[53],[55] Overlying epidermis is thinned out with occasional civatte bodies [Figure - 3].
 |
| Figure 3: Lichen nitidus: Section from papule showing well circumscribed mixed cell infiltrate in close proximity of epidermis and confined to papillary dermis (H and E, ×100) |
Lichen striatus
This, on the other hand, displays papular lesions in a linear, unilateral fashion often following Blaschko′s lines, usually occurring in adolescents especially females. [56],[57],[58] Its histopathology is marked by hyperkeratosis, parakeratosis, often minute intraepidermal vesicles containing Langerhan′s cells and less dense infiltrate of lymphocyte, histiocytes, and melanophages in the mildly edematous dermal papillae [29],[56],[59],[60],[61] [Figure - 4]. Hard et al., [61] believe that linear lichen planus and lichen striatus are the opposite ends of a spectrum.
 |
| Figure 4: Lichen striatus: Section show features mimicking lichen planus but are focal and may be missed without step sections (H and E, ×40) |
Lichen planus-like keratosis
They are benign lichenoid keratosis present as sudden eruption of solitary or a few violaceous, rusty lesions with thin scale usually present on the arms or presternal areas of middle aged/elderly women. [62],[63],[64] The microscopic features are pathognomonic characterized by florid lichenoid reaction, prominent pigment incontinence, and numerous civatte bodies. The dense infiltrate of lymphocytes and macrophages may also show a few plasma cell and eosinophilis. [65] Individual histopathologic variations prompted Jang et al., [66] to classify lichenoid keratosis in three groups, namely, lichen planus-like, seborrheic keratosis-like, and lupus erythematosus-like lichenoid keratosis. The salient histopathological features of the preceding lichenoid interface dermatoses are outlined [Table - 2].
Twenty-nail dystrophy
Trachyonychia, a fascinating clinical condition, was brought to focus 25 years ago. Ever since, it has been sparingly reported. Nonetheless, the condition is well recognized, and its diagnosis is made on the basis of clinical features characterized by [67],[68] onset in infancy/childhood, and occasionally in adults. The lesions are fairly representative, and are characterized by the alternating elevation and depression (ridging) and/or pitting, lack of luster, roughening likened to sandpaper, splitting, and change to a muddy grayish-white color. Dystrophy is prominent. Several modes of occurrence have been described including an hereditary component. The confirmation of diagnosis is through microscopic pathology corresponding to endogenous eczema/dermatitis, lichen-planus-like or psoriatic-form. It is a self-limiting condition and may occasionally require intervention.
Drug Induced Lichenoid Dermatitis
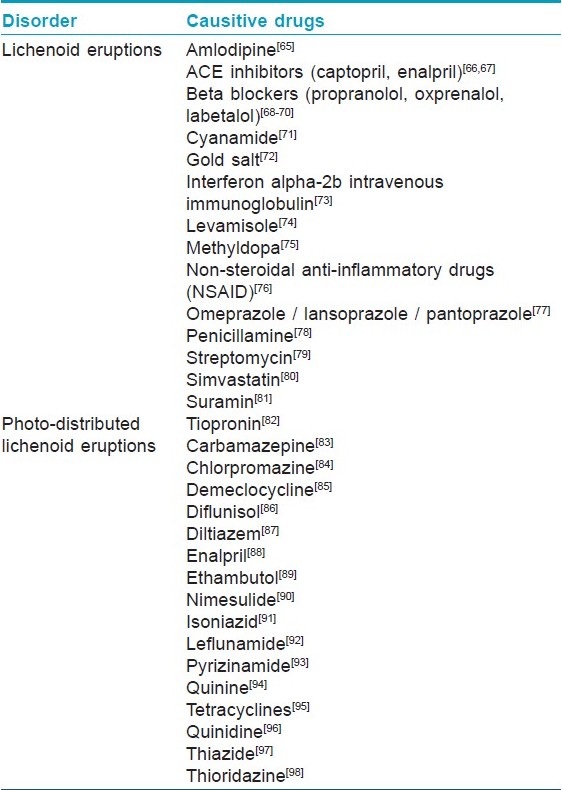
The in vogue term, lichenoid drug eruptions, is an often encountered drug reaction to a heterogeneous group of ingested and/or injected drugs used in a wide variety of systemic disorders. Ever since the observation of lichen planus-like eruptions occurring in troops who took mepacrine in the World War II, [69] numerous reports [70],[71],[72],[73],[74],[75],[76],[77],[78],[79],[80],[81],[82],[83],[84],[85],[86],[87],[88],[89],[90],[91],[92],[93],[94],[95],[96],[97],[98],[99],[100],[101],[102],[103] have recorded this entity in response to different drugs [Table - 3]. Wechsler [104] initially reported photo-lichenoid dermatitis in the year 1954, as a photo allergic reaction to drug(s), presenting a lichenoid pattern on clinical as well as histopathological examination. The lichenoid eruptions/photo-lichenoid eruptions clinically closely mimic lichen planus, but may have some eczematous element and usually leave a pronounced residual pigmentation. Histopathologically, differentiating features of lichenoid eruptions include foci of parakeratosis, mild basal vacuolar changes with a few eosinophils/plasma cells. The degree of melanin incontinence is higher in lichenoid eruption in contrast that of lichen planus [105] [Figure - 5]. However, the dermal infiltrate is less dense and less band-like. Photo-lichenoid eruptions, on the other hand, may closely mimic lichen planus. [106]
 |
| Figure 5: Lichenoid drug eruption: Section showing lichenoid infiltrate similar to lichen planus, but with more numerous eosinophils, parakeratosis and perivascular distribution of infiltrate (H and E, ×200) |
Fixed drug eruptions
A wide variety of drugs have been incriminated. [107] They may probably be induced by drug acting as hapten, binding to keratino/melanocytes producing an immunological reaction, an antibody-dependent cellular cytoid response. Suppressor/cytotoxic lymphocytes attack the drug altered epidermal cells causing the eruption, and thus retain the cutaneous memory in cases of repeated offence by the drug. [107],[108],[109] The clinical lesions may mimic lichenoid interface dermatoses. [107] The microscopic pathology of fixed drug eruptions (FDE) shows a prominent vacuolar change in the basal cells, civatte bodies, melanin incontinence, and inflammatory infiltrate often comprising neutrophils approximating the dermo-epidermal junction, extending up to mid-epidermis and dermis. [107],[108],[109],[110]
Erythema multiforme and toxic epidermal necrolysis
They are other severe forms of drug eruptions. Histopathology shows changes that of lichenoid dermatitis, conforming to either epidermal, dermal, or mixed pattern. It is characterized by mild-to-moderate lymphocytic infiltrate, a few macrophages, obscuring dermo-epidermal junction, and surrounding the dermal blood vessels up to mid-dermis. Apoptosis with prominent epidermal cell death extending beyond basal cell layer [111],[112],[113] is another salient feature. TEN, on the other hand, may reveal a sub-epidermal bulla beneath a confluent epidermal necrosis. Lymphocytic infiltrate is sparse, and perivascular. Sweat ducts are often involved, and may show a basal cell apoptosis resulting even in necrosis. [114],[115],[116],[117]
Special Forms of Lichenoid Dermatitis
Acquired immunodeficiency syndrome related lichenoid dermatitis
It has been a controversial, infrequently encountered entity. [29] An increased prevalence and severity of cutaneous photosensitivity has been recognized in human immunodeficiency virus (HIV) infection. Lichenoid and/or nonlichenoid eczematous are the two distinct clinical manifestations. Burger and Dhar [118] have studied lichenoid photo eruptions in HIV infection. Systemic and cutaneous immune abnormalities may be relevant in their pathogenesis. [119] Histopathology largely shows a lichenoid reaction pattern depicting interface changes, resembling those of EM/ FDE. [29],[119]
Lichenoid reaction to graft versus host disease
Chronic graft versus host disease occurring after 3 months of transplantation or later may resemble lichenoid reactions, affecting the palms, soles, trunk buttocks, and thighs. Oral ulcers and xerostomia may be its accompaniment. The microscopic pathology of the chronic phase may resemble that of lichen planus albeit marked by a dense inflammatory infiltrate, and prominent pigment incontinence. Small foci of ′′columnar epidermal necrosis′′ may also be a prominent feature. [29],[120],[121],[122]
Lichenoid eruptions in paraneoplastic pemphigus
They may either occur independently or on previously blistered skin. They are invariably accompanied by severe stomatitis. As the disease gets chronic or after treatment the lichenoid eruptions may overtake the blistering. Unlike, pemphigus vulgaris, they are often seen on the palms, soles, and over paronychial tissue. [123] The microscopic findings resemble EM with lichenoid tissue reaction. Dyskeratotic cell at different level of epidermis is another feature. Subepidermal as well as suprabasal cleft depicting acantholysis have also been recorded. [29],[124]
Lichenoid dermatitis in lupus erythematosus
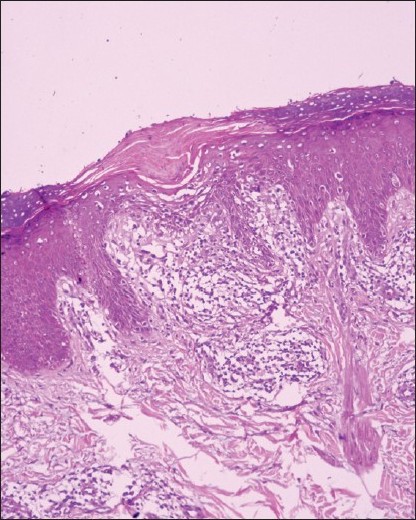
A lichenoid reaction pattern in variable permutation and combination is a common denominator. The clinical features and variants of lupus erythematosus (LE) have been extensively recorded. [123] Some degree of overlap may be seen in its different clinical variants. Discoid lupus erythematosus (DLE) displays a lichenoid reaction pattern with chiefly a peripilosebaceous/follicular superficial and deep dermal lymphocytic infiltrate. Liquefaction degeneration, scattered civatte bodies, hyperkeratosis, atrophic malpighian layer, and keratotic plugging are succinctly observed [125],[126] [Figure - 6]. Direct immunofluorescence of involved skin reveals the deposition of IgG and IgM along the basement membrane zone in most cases. The cutaneous lesions of SLE show vacuolar degeneration of the basement membrane, yet civatte bodies are unusual. Fibrinoid material can be deposited in dermis around capillaries and interstitium, which may cause thickening of the basement membrane zone. Special stains may reveal deposition of mucin. Hematoxyphilic bodies, which are usual in the visceral lesions, are rare in the skin lesions. A positive lupus band test is an additional pointer towards diagnosis, which is invariably positive in involved skin. [125],[127],[128]
 |
| Figure 6: Lupus erythematosus: Section showing hyperkeratosis with follicular plugging with thinning and flattening of epithelium and focal thickening of basement membrane. A predominantly lymphocytic infiltrate is seen around the hair follicles and along dermo--epidermal junction (H and E, ×40) |
The subacute lupus erythematosus displays a wide range of clinical expressions and mild systemic/serological abnormalities. [29],[123] The histopathological features of cutaneous lesions, however, reveal most of the features seen in discoid lupus but with more basal vacuolar changes, epidermal atrophy, dermal edema and superficial mucin in the former. Compared to discoid lupus, it has less pronounced hyperkeratosis, keratotic plugging, pilo-sebaceous atrophy, basement membrane thickening, and cellular infiltrate. [129],[130],[131]
Miscellaneous Disorders Showing Lichenoid Dermatitis
Late secondary syphilis
Its histopathology may display a lichenoid reaction pattern, the inflammatory infiltrate formed primarily by plasma cells, which are distributed through out the dermis. [1]
Gianotti-Crosti syndrome
It is an uncommon, self-limited, acrodermatitis of childhood, characterized by an erythematous papular eruptions symmetrically distributed on the face and limbs with mild lymphadenopathy. It is thought to be of viral origin. The histopathologic findings are nonspecific, and include focal parakeratosis, mild spongiosis, superficial perivascular infiltrate, papillary dermal edema, and extravasated red blood cells. Interface changes with some basal vacuolization may be present. [132]
Herpes simplex virus (HSV) and varicella-zoster virus (VZV)
They are responsible for various atypical mucocutaneous manifestations in the immunosuppressed population. An altered virus-host cell relationship may be one of the pathomachanisms. Histopathology reveals lichenoid dermatitis. Specific HSV-1, HSV-2, and VZV in situ hybridization proved the viral origin of the cutaneous lesions. [133]
Pityriasis lichenoides et varioliformis acuta (PLEVA)
It may show a heavy lymphocytic infiltrate obscuring the dermo-epidermal junction with focal epidermal cell death, and confluent epidermal necrosis. A wedge-shaped dermal infiltrate with apex in deep dermis with variable hemorrhage may be diagnostic. [134]
Poikilodermatous disorders
They are heterogeneous group of disorders, characterized by erythema, mottled pigmentation and epidermal atrophy, complimented histologically by basal vacuolar changes, melanin incontinence and telangiectasia of superficial dermal vessels. [5],[29],[123] The genodermatoses-like Rothmund-Thomson syndrome, Blooms syndrome and dyskeratosis congenital reveal their independent clinical characteristic, and histopathological peculiarities, but with a variable degree of lichenoid reaction. Poikiloderma atrophicans vasculare may represent an early stage of mycosis fungoides. [29],[123] Poikiloderma of civatte is now disputed as a distinct entity. [135] Some poikilodermas may be related, in some ways to a graft versus host reaction. [136]
Dermatomyositis
Skin lesions have shown a spectrum of histopathological changes, varying from sparse perivascular lymphocytic infiltrate, edema, mucinous changes in the upper dermis, to full-fledged lichenoid reaction pattern with prominent basal vacuolar changes. Occasional civatte bodies and/or neutorphils can be an accompaniment. Severe cases resemble acute lupus erythematosus. Infrequently poikilodermatous features can be an additional with dilated superficial blood vessels and pigment incontinence. Lupus band test is usually negative, although colloid bodies containing IgM may be a salient feature in papillary dermis. [137],[138],[139]
Lichen sclerosus (LS)/ lichen sclerosus et atrophicus/balanitis xerotica obliterans/kraurosis vulvae
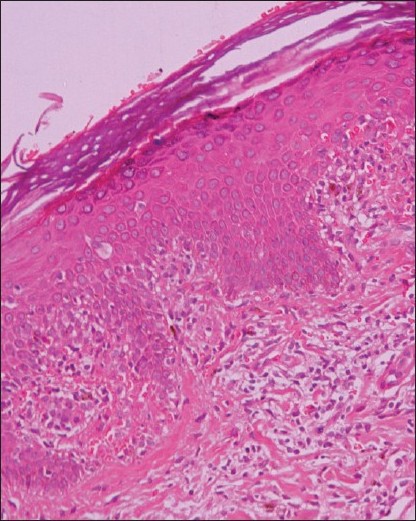
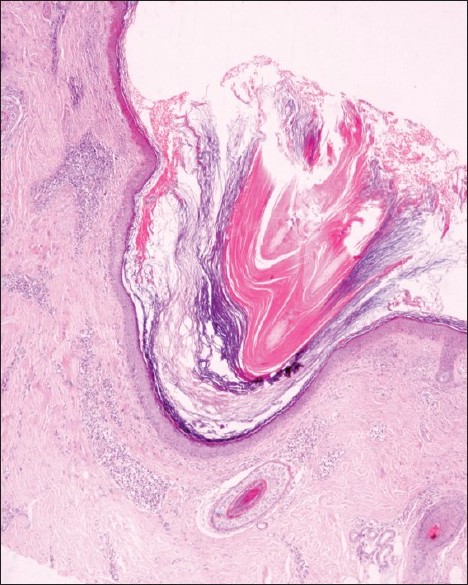
It is a chronic inflammatory dermatosis that results in white plaques with epidermal atrophy. It appears to begin as an interface dermatitis. Its early lesions may show a heavy infilammatory infiltrate with vacuolar changes, and apoptotic basal changes. As the disease progresses, the infiltrate is eventually pushed downwards by expanding zone of edema and sclerosis [29] [Figure - 7].
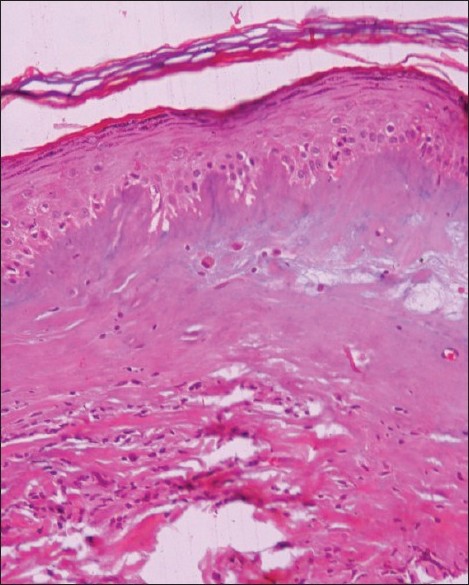 |
| Figure 7: Lichen sclerosus and atrophicus: Section showing hyperkeratosis with atrophy of stratum malphigii, prominent edema, and homogenization of collagen in upper dermis. Early lesion may show interface dermatitis with superficial inflammation in direct contact with epidermis which soon gets separated by edema. (H and E, ×100) |
Lichenoid contact dermatitis
It shows a patchy band-like dermal infiltrate of lymphocytes with a few eosinophils and a mild basal spongiosis. It usually results from contact with rubber and chemical used in clothing dyes and wine industries. [29]
Progressive pigmented purpuric dermatosis/Schamberg′s disease
It is a chronic discoloration of the skin, which usually affects the legs and often spreads slowly. It may show lichenoid reaction pattern. However, the presence of purpura and deposits of hemosiderin distinguish it from other disorders. [5],[29]
Erythroderma and lichen amyloidosis may have prominent pigmented lichenoid tissue reaction. [5],[29],[123]
The latter is recognized by hyperpigmented, lichenified and hyperkeratotic well-formed lesions. [140] Pathologic changes in the form of acanthotic and hyperkeratotic epidermis is cardinal in lichenoid lesions. Eosinophilic cytoid bodies in the epidermis are diagnostic, following histo-chemical stains like congo-red and crystal violet [Figure - 8]. The eruption of lymphocyte recovery, initially recorded by Home et al., [141] are now believed to be a form of graft-versus-host disease. [142]
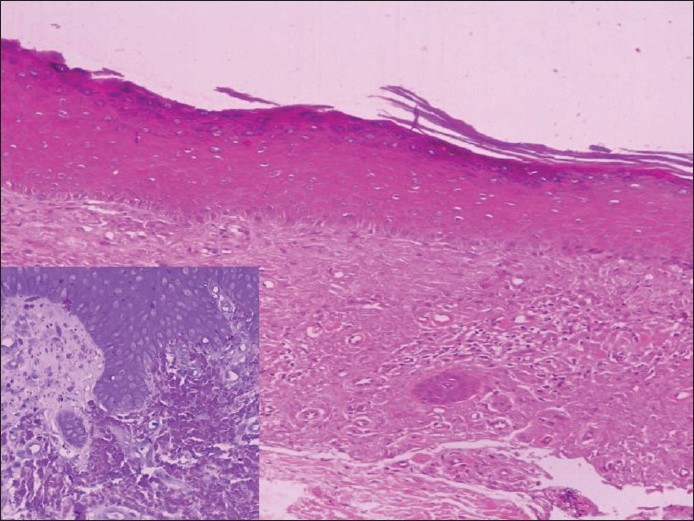 |
| Figure 8: Lichen amyloidosis: Section from lichen amyloidosis showing large acellular homogenous deposits of amyloid in papillary dermis, confirmed on special stains (crystal violet, inset). Smaller amounts of deposits can mimic colloid bodies of lichen planus (H and E, ×100) |
Lichen aureus, a variant of pigmented purpuric dermatoses (PPD) is known for persistent, golden, copper-colored, flat-topped papules that appear suddenly. Minute cutaneous blood vassels are the prime target [143],[144] [Figure - 9].
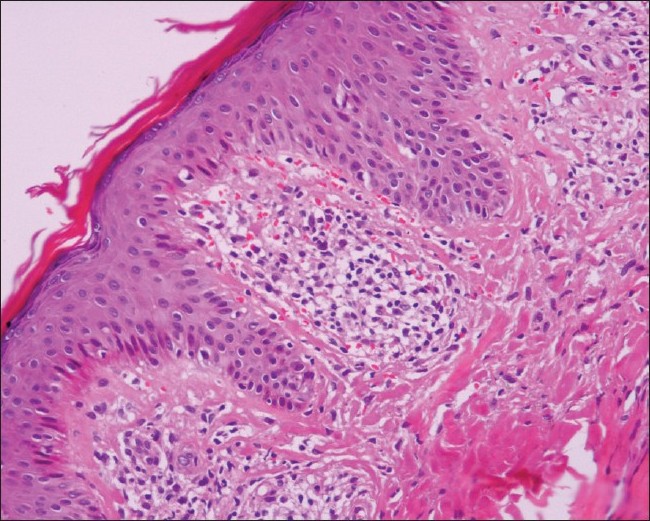 |
| Figure 9: Lichen aureus: Section shows moderate inflammatory infiltrate around the papillary dermal vessels which can cause focal interface dermatitis. Extravasated red blood cells are prominent (H and E, ×200) |
Lichen spinulosus
It is characterized by round-to-oval patches of grouped follicular papules with rough keratotic centers [145] may yet be another entity, which requires confirmation by microscopic pathology evident as a keratotic plug consisting of laminated corneocytes, occupying a dilated follicle.
Conclusions
It is worthwhile, at this point in time, to recognize lichenoid tissue reaction/interface dermatitis as an exclusive clinical and/or pathological entity, which has several dermatoses of heterogeneous nature under its ever enlarging domain. Accordingly, it was considered imperative to recapture the precise clinical as well as pathological overtones to exercise the relevant treatment modality.
| 1. |
Tilly JJ, Drolat BA, Esterly NB. Lichenoid eruptions in children. J Am Acad Dermatol 2004;51:606-24.
[Google Scholar]
|
| 2. |
Shiohara T, Moriya N, Nagashima M. The lichenoid tissue reaction. A new concept of pathogenesis. Int J Dermatol 1988;27:365-74.
[Google Scholar]
|
| 3. |
Crowson AN, Magro CM, Mihm MC Jr. Interface Dermatitis. Arch Pathol Lab Med 2008;132:652-66.
[Google Scholar]
|
| 4. |
Goeckerman WH, Montogomery H. Lupus eryhtematosus: An evaluation of histopathologic examination. Arch Dermatol 1932;25:304-16.
[Google Scholar]
|
| 5. |
Pinkus H. Lichenoid tissue reactions. A speculative review of the clinical spectrum of epidermal basal cell damage with special reference to erythema dyschromicum perstans. Arch Dermatol 1973;107:840-6.
[Google Scholar]
|
| 6. |
Montgomery H. Dermatopathology. New York: Harper and Row Publishers; 1967.
[Google Scholar]
|
| 7. |
Samman PD. Lichen planus and lichenoid eruptions. In: Rook A, Wilkinson DS, Ebling FJ, editors. Textbook of Dermatology. Oxford, England: Blackwell Scientific Publications; 1968. p. 1194-212.
[Google Scholar]
|
| 8. |
Hirsch P, Marmelzat WL. Lichenoid actinic keratosis. Deramtol Internationalis 1967;6:101-3.
[Google Scholar]
|
| 9. |
Shapiro L, Ackerman AB. Solitary lichen planus-like keratosis. Dermatologica 1966;132:386-92.
[Google Scholar]
|
| 10. |
Lever WF. Histopathology of the skin. 4 th ed. Philadelphia: JB Lippincott Co; 1967. pp. 255-6.
[Google Scholar]
|
| 11. |
Katzenellenbogen I. Lichen planus actinicus (lichen planus in subtropical countries). Dermatologica 1962;124:10-20.
[Google Scholar]
|
| 12. |
El-Zawahari M. Lichen planus tropicus. Dermatol Internationalis 1965;4:92-5.
[Google Scholar]
|
| 13. |
Hague JS, Ilchyshn A. Lichenoid photosensitive eruption due to capecitabine chemotherapy for matastatic breast cancer. Clin Exp Dermatol 2007;32:102-3.
[Google Scholar]
|
| 14. |
Patterson JW. The spectrum of lichenoid dermatitis. J Cutan Pathol 1991:18:67-74.
[Google Scholar]
|
| 15. |
Hashimoto K. Apoptosis in lichen planus and several other dermatoses. Intra-epidermal cell death with filamentous degeneration. Acta Derm Venereol 1976;56:187-210.
[Google Scholar]
|
| 16. |
Shai A, Halevy S. Lichen Planus and lichen planus-like eruptions: Pathogenesis and associated diseases. Int J Dermatol 1992;31:379-84.
[Google Scholar]
|
| 17. |
Bennion SD, Middleton MH, David-Bajar KM, Brice S, Norris DA. In three types of interface dermatitis, different patterns of expression of intercellular adhesion molecule-I (ICAM-I) indicate different triggers of disease. J Invest Dermatol 1995;105:71S-79S.
[Google Scholar]
|
| 18. |
Oliver GF, Winkelmann RK, Muller SA. Lichenoid dermatitis: A clinicopathologic and immunopathologic review of sixty-two cases. J Am Acad Dermatol 1989;21:284-92.
[Google Scholar]
|
| 19. |
Okamoto H, Mizuno K, Itoh T, Tanaka K, Horio T. Evaluation of apoptotic cells induced by ultraviolet light B radiation in epidermal sheets stained by the TUNEL technique. J Invest Dermatol 1999;113:802-7.
[Google Scholar]
|
| 20. |
Iijima W, Ohtani H, Nakayama T, Sugawara Y, Sato E, Nagura H, et al. Infiltrating CD8+ T cells in oral lichen planus predominantly express CCR5 and CXCR3 and carry respective chemokine ligands RANTES/CCL5 and IP10/CXCL10 in their cytolytic granules: A potential self-recruiting mechanism. Am J Pathol 2003;163:261-8.
[Google Scholar]
|
| 21. |
Lodi G, Scully C, Carrozzo M, Griffiths M, Sugerman PB, Thongprasom K. Current controversies in oral lichen planus; a report of an international consensus meeting: Part 1. Viral infections and aetiopathogenesis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100:40-51.
[Google Scholar]
|
| 22. |
Sugerman PB, Savage NW, Walsh LJ, Zhao ZZ, Zhou XJ, Khan A, et al. The pathogenesis of oral lichen planus. Crit Rev Oral Biol Med 2002;13:350-65.
[Google Scholar]
|
| 23. |
Podack ER. Lymphocyte mediated cytotoxicity. In: Preissner KT, Rosenblatt S, Mosher DF, editors. Biology of Vitronectins and their receptors. Amsterdam: Elsevier; 1993. p. 237-42.
[Google Scholar]
|
| 24. |
Podack ER. Execution and suicide: Cytotoxic lymphocytes enforce draconian laws through separate molecular pathways. Curr Opin Immunol 1995:7:11-6.
[Google Scholar]
|
| 25. |
Shimizu M, Higaki Y, Higaki M, Kawashima M. The role of granzyme B-expressing CD8-positive T cells in apoptosis of keratinocytes in lichen planus. Arch Dermatol Res 1997;289:527-32.
[Google Scholar]
|
| 26. |
Prpiæ Massari L, Kastelan M, Gruber F, Laskarin G, Sotosek Tokmadziæ V, Strbo N, et al . Perforin expression in peripheral blood lymphocytes and skin-infiltrating cells in patients with lichen planus. Br J Dermatol 2004;151:433-9.
[Google Scholar]
|
| 27. |
Shiohara T, Mizukawa Y. The immunological basis of lichenoid tissue reaction . Autoimmun Rev 2005;4:236-41.
[Google Scholar]
|
| 28. |
Mizukawa Y, Shiohara T. Fixed drug eruption: A prototypic disorder mediated by effector memory T cells. Curr Allergy Asthma Rep 2009;9:71-7.
[Google Scholar]
|
| 29. |
Weedon D. The Lichenoid Reaction Pattern. In: Weedon D, editor. Skin Pathology. 2 nd ed. New York: Churchill Livingstone; 2002. p. 31-74.
[Google Scholar]
|
| 30. |
Hamanaka H, Mizutani H, Shimizu M. Sparfloxacin-induced photosensitivity and the occurrence of a lichenoid tissue reaction after prolonged exposure. J Am Acad Dermatol 1998;38:945-9.
[Google Scholar]
|
| 31. |
Sontheimer RD. Lichenoid tissue reaction/interface dermatitis: Clinical and histological perspectives. J Invest Dermatol 2009;129:1088-99.
[Google Scholar]
|
| 32. |
Scalf LA, Fowler JF Jr, Morgan KW, Looney SW. Dental metal allergy in patients with oral, cutaneous, and genital lichenoid reactions. Am J Contact Dermat 2001;12:146-50.
[Google Scholar]
|
| 33. |
Giuliani M, Lajolo C, Sartorio A, Scivetti M, Capodiferro S, Tumbarello M. Oral lichenoid lesions in HIV-HCV-coinfected subjects during antiviral therapy: 2 cases and review of the literature. Am J Dermatopathol 2008;30:466-71.
[Google Scholar]
|
| 34. |
Leitman SF, Tisdale JF, Bolan CD, Popovsky MA, Klippel JH, Balow JE, et al. Transfusion-associated GVHD after fludarabine therapy in a patient with systemic lupus erythematosus. Transfusion 2003;43:1667-71.
[Google Scholar]
|
| 35. |
Sanchez-Perez J, Rios Buceta L, Fraga J, García- Díez A. Lichen planus with lesions on the palms and/or soles; prevalence and clinicopathological study of 36 patients. Br J Dermatol 2000;142:310-4.
[Google Scholar]
|
| 36. |
Ellgehausen P, Elsner P, Berger G. Drug induced lichen planus. Clin Dermatol 1998;16:325-32.
[Google Scholar]
|
| 37. |
Irvine C. Irvine F. Champion RH. Long-term follow-up of lichen planus. Acta Derm Venereol 1991;71:242-4.
[Google Scholar]
|
| 38. |
Ragaz A, Ackerman AB. Evolution, maturation, and regression of lesions of lichen planus. New observations and correlations of clinical and histologic findings. Am J Dermatopathol 1981;3:5-25
[Google Scholar]
|
| 39. |
Ebner H, Gebhart W. Epidermal changes in lichen planus. J Cutan Pathol 1976;3:167-74.
[Google Scholar]
|
| 40. |
Rippis GE, Becker B, Scott G. Hypertrophic lichen planus in three HIV-positive patients: A histologic and immunological study. J Cutan Pathol 1994;21:52-8.
[Google Scholar]
|
| 41. |
Hartl C, Steen KH, Wegner H, Seifert HW, Bieber T. Unilateral linear lichen planus with mucous membrane involvement. Acta Derm Venereol 1999;79:145-6.
[Google Scholar]
|
| 42. |
Friedman DB, Hashimoto K. Annular atrophic lichen planus. J Am Acad Dermatol 1991;25:392-4.
[Google Scholar]
|
| 43. |
Long CC, Finalay AY. Multiple linear lichen planus in the lines of Blaschko. Br J Dermatol 1996;135:275-6.
[Google Scholar]
|
| 44. |
Salman SM, Kibbi AG, Zaynoun S. Actinic lichen planus. A clinicopathologic study of 16 patients. J Am Acad Dermatol 1989;20:226-31.
[Google Scholar]
|
| 45. |
Eisen D. The vulvovaginal-gingival syndrome of lichen planus. The clinical characteristics of 22 patients. Arch Dermatol 1994;130:1379-82.
[Google Scholar]
|
| 46. |
Lewis FM, Shah M, Harrington CI. Vulval involvement in lichen planus: A study of 37 women. Br J Dermatol 1996;135:89-91.
[Google Scholar]
|
| 47. |
Vente C, Reich K, Rupprecht R, Neumann C. Erosive Mucosal lichen planus: Response to topical treatment with tacrolimus. Br J Dermatol 1999;140:338-42.
[Google Scholar]
|
| 48. |
Crotty CP, Su WP, Winkelmann RK. Ulcerative lichen planus. Follow-up of surgical excision and grafting. Arch Dermatol 1980;116:1252-6.
[Google Scholar]
|
| 49. |
Lapins NA, Willoughby C, Helwig EB. Lichen nitidus. A study of forty-three cases. Cutis 1978;21:634-7.
[Google Scholar]
|
| 50. |
Chen W, Schramm M, Zouboulis CC. Generalized lichen nitidus. J Am Acad Dermatol 1997;36:630-1.
[Google Scholar]
|
| 51. |
Bettoli V, De Padova MP, Corazza M, Virgili A. Generalized lichen nitidus with oral and nail involvement in a child. Dermatology 1997;194:367-9.
[Google Scholar]
|
| 52. |
Smoller BR, Flynn TC. Immunohistochemical examination of lichen nitidus suggests that it is not a localized popular variant of lichen planus. J Am Acad Dermatol 1992;27:232-6.
[Google Scholar]
|
| 53. |
Clausen J, Jacobsen FK, Brandrup F. Lichen nitidus: Electron microscopic and immunofluorescent studies. Acta Derm Venereol 1982;62:15-9.
[Google Scholar]
|
| 54. |
Hussain K. Summertime actinic lichenoid eruption a distinct entity, should be termed actinic lichen nitidus. Arch Dermatol 1998;134:1302-3.
[Google Scholar]
|
| 55. |
Khopkar U, Joshi R. Distinguishing lichen scrofulosorum from lichen nitidus. Dermatopathol: Pract Concept 1999;5:44-5.
[Google Scholar]
|
| 56. |
Zhang Y, McNutt NS. Lichen striatus. Histological, immunohistochemical, and ultrastructural study of 37 cases. J Cutan Pathol 2001;28:65-71.
[Google Scholar]
|
| 57. |
Ciconte A, Bekhor P. Lichen striatus following solarium exposure. Australas J Dermatol 2007;48:99-101.
[Google Scholar]
|
| 58. |
Taieb A, El Youbi A, Grosshans E, Maleville J. Lichen striatus: A Blaschko linear acquired inflammatory skin eruption. J Am Acad Dermatol 1991;25:637-42.
[Google Scholar]
|
| 59. |
Reed RJ, Meek T, Ichinose H. Lichen striatus: A model for the histologic spectrum of lichenoid reactions. J Cutan Pathol 1975;2:1-18.
[Google Scholar]
|
| 60. |
Gianotti R, Restano L, Grimalt R, Berti E, Alessi E, Caputo R. Lichen striatus--a chameleon: An histopathological and immunohistological study of forty-one cases. J Cutan Pathol 1995;22:18-22.
[Google Scholar]
|
| 61. |
Rose C, Hauber K, Starostik P. Lichen striatus: A clinicopathologic study with follow-up in 13 patients. Am J Dermatopathol 2000;22:354.
[Google Scholar]
|
| 62. |
Herd RM, McLaren KM, Aldridge RD. Linear lichen planus and lichen striatus-opposite ends of a spectrum. Clin Exp Dermatol 1993;18:335-7.
[Google Scholar]
|
| 63. |
Prieto VG, Casal M, McNutt NS. Lichen planus-like keratosis. A clinical and histological reexamination. Am J Surg Pathol 1993;17:259-63.
[Google Scholar]
|
| 64. |
Goldenhersh MA, Barnhill RL, Rosenbaum HM, Stenn KS. Documented evolution of a solar lentigo into a solitary lichen planus-like keratosis. J Cutan Pathol 1986;13:308-11.
[Google Scholar]
|
| 65. |
Berger TG, Graham JH, Goette DK. Lichenoid benign keratosis. J Am Acad Dermatol 1984;11:635-8.
[Google Scholar]
|
| 66. |
Jang KA, Kim SH, Choi JH, Sung KJ, Moon KC, Koh JK. Lichenoid keratosis: A clinicopathologic study of 17 patients. J Am Acad Dermatol 2000;43:511-6.
[Google Scholar]
|
| 67. |
Sehgal VN. Twenty nail dystrophy trachyonychia: An overview. J Dermatol 2007;34:361-6.
[Google Scholar]
|
| 68. |
Yokozeki H, Niiyama S, Nishioka K. Twenty-nail dystrophy (trachyonychia) caused by lichen planus in a patient with gold allergy. Br J Dermatol 2005;152:1087-9.
[Google Scholar]
|
| 69. |
Bauer F. Quinacrine hydrochloride drug eruption (topical lichenoid dermatitis). Its early and late sequelae and its malignant potiential: A review. J Am Acad Dermatol 1981;4:239-48.
[Google Scholar]
|
| 70. |
Swale VJ, McGregor JM. Amlodipine-associated lichen planus. Br J Dermatol 2001;144:920-21.
[Google Scholar]
|
| 71. |
Phillips WG, Vaughan-Jones S, Jenkins R, Breathnach SM. Captopril-induced lichenoid eruption. Clin Exp Dermatol 1994;19:317-20.
[Google Scholar]
|
| 72. |
Roten SV, Mainetti C, Donath R, Saurat JH. Enalapril-induced lichen planus-like eruption. J Am Acad Dermatol 1995;32:293-5.
[Google Scholar]
|
| 73. |
Hawk JL. Lichenoid drug eruption induced by propanolol. Clin Exp Dermatol 1980;5:93-6.
[Google Scholar]
|
| 74. |
Gange RW, Levene GM. A distinctive eruption in patients receiving oxyprenalol. Clin Exp Dermatol 1979;4:87-97.
[Google Scholar]
|
| 75. |
Gange RW, Jones EW. Bullous lichen planus caused by labetalol. Br Med J 1978;1:816-7.
[Google Scholar]
|
| 76. |
Aguilar A, Gallego MA, Pigue E. Lichenoid drug eruption due to cynamide. Int J Dermatol 1999;38:950-1.
[Google Scholar]
|
| 77. |
Penneys NS, Ackerman AB, Gottlieb NL. Gold dermatitis. A clinical and histopathological study. Arch Dermatol 1974;109:372-6.
[Google Scholar]
|
| 78. |
Yockey SM, Ahmed I. Intravenous immunoglobulin-induced lichenoid dermatitis: A unique adverse reaction. Mayo Clin Proc 1997;72:1151-2.
[Google Scholar]
|
| 79. |
Kirby JD, Black M, McGibbon D. Levamsole-induced lichenoid eruptions. J R Soc Med 1980;73:208-11.
[Google Scholar]
|
| 80. |
Cutler TP. Lichen planus caused by pyrimethamine. Clin Exp Dermatol 1980;5:253-6.
[Google Scholar]
|
| 81. |
Ozkan S, Izler F, Fetil E, Dorak F, Güneº T. Naproxen-induce lichen planus bullosus. Acta Derm Venereol 1999;79:329-30.
[Google Scholar]
|
| 82. |
Bong JL, Lucke TW, Douglas WS. Lichenoid drug eruption with proton pump inhibitors. BMJ 2000;320:283.
[Google Scholar]
|
| 83. |
Van Hecke E, Kint A, Temmerman L. A lichenoid eruption induced by penicillamine. Arch Dermatol 1981;117:676-7.
[Google Scholar]
|
| 84. |
Fellner MJ. Lichen planus. Int J Dermatol 1980;19:71-5.
[Google Scholar]
|
| 85. |
Roger D, Rolle F, Labrousse F, Brosset A, Bonnetblanc JM. Simvastatin-induced lichenoid drug eruption. Clin Exp Dermatol 1994;19:88-9.
[Google Scholar]
|
| 86. |
Lowitt MH, Eisenberger M, Sina B, Kao GF. Cutaneous eruptions from suramin. A clinical and histopathologic study of 60 patients. Arch Dermatol 1995;131:1147-53.
[Google Scholar]
|
| 87. |
Pierard E, Delaporte E, Flipo RM, Duneton-Bitbol V, Dejobert Y, Piette F, et al. Tiopronin-induced lichenoid eruption. J Am Acad Dermatol 1994;31:665-7.
[Google Scholar]
|
| 88. |
Yasuda S, Mizuno N, Kawabe Y, Sakakibara S. Photosensitive lichenoid reaction accompanied by nonphotosensitive subacute prurigo caused by carbamazepine. Photodermatol 1988;5:206-10.
[Google Scholar]
|
| 89. |
Matsuo I, Ozawa A, Niizuma K, Ohkido M. Lichenoid dermatitis due to chlorpromazine phototoxicity. Dermatologica 1979;159:46-9.
[Google Scholar]
|
| 90. |
Jones HE, Lewis CW, Reisner JE. Photosensitive lichenoid eruption associated with demeclocycline. Arch Dermatol 1972;106:58-63.
[Google Scholar]
|
| 91. |
Street ML, Winkelmann RK. Lichenoid photoreactive epidermal necrosis with diflunisal. J Am Acad Dermatol 1989;20:850-1.
[Google Scholar]
|
| 92. |
Scherschun L, Lee MW, Lim HW. Diltiazem-associated photodistributed hyperpigmentation: A review of 4 cases. Arch Dermatol 2001;137:179-82.
[Google Scholar]
|
| 93. |
Kanwar AJ, Dhar S, Ghosh S. Photosensitive lichenoid eruption due to enalapril. Dermatology 1993;187:80.
[Google Scholar]
|
| 94. |
Grossman ME, Warren K, Mady A, Satra KH. Lichenoid eruption associated with ethambutol. J Am Acad Dermatol 1995;33:675-6.
[Google Scholar]
|
| 95. |
Tursen U, Kaya TI, Kokturk A, Dusmez D. Lichenoid photodermatitis associated with nimesulide. Int J Dermatol 2001;40:767-8.
[Google Scholar]
|
| 96. |
Lee AY, Jung SY. Two patients with isoniazid-induced photosensitive lichenoid eruptions confirmed by photopatch test. Photodermatol Photoimmunol Photomed 1998;14:77-8.
[Google Scholar]
|
| 97. |
Rivarola de Gutierrez E, Abaca H. Photodistributed lichenoid drug eruption with rhabdomyolysis occurring during leflunomide therapy. Dermatology 2004;208:232-3.
[Google Scholar]
|
| 98. |
Choonhakarn C, Janma J. Pyrazinamide-induced lichenoid photodermatitis. J Am Acad Dermatol 1999;40:645-6.
[Google Scholar]
|
| 99. |
Dawson TA. Quinine lichenoid photosensitivity. Clin Exp Dermatol 1986;11:670-1.
[Google Scholar]
|
| 100. |
Wolf R, Oumeish OY. Photodermatoses. Clin Dermatol 1998;16:41-57.
[Google Scholar]
|
| 101. |
Wolf R, Dorfman B, Krakowski A. Quinidine-induced lichenoid and eczematous photodermatitis. Dermatologica 1987;174:285-9.
[Google Scholar]
|
| 102. |
Johnston GA. Thiazide-induced lichenoid photosensitivity. Clin Exp Dermatol 2002;27:670-2.
[Google Scholar]
|
| 103. |
Llambrich A, Lecha M. Photoinduced lichenoid reaction by thioridazine. Photodermatol Photoimmunol Photomed 2004;20:108-9.
[Google Scholar]
|
| 104. |
Wescsler HL. Dermatitis medicamentosa; a lichen-planus-like eruption due to quinidine. AMA Arch Dermatol Syphilol 1954;69:741-4.
[Google Scholar]
|
| 105. |
Hawk JL. Lichenoid drug eruption induced by propanolol. Clin Exp Dermatol 1980;5:93-96.
[Google Scholar]
|
| 106. |
West AJ, Berger TG, LeBoit PE. A comparative histopathologic study of photodistributed and nonphotodistributed lichenoid drug eruptions. J Am Acad Dermatol 1990;23:689-93.
[Google Scholar]
|
| 107. |
Sehgal VN, Srivastava G. Fixed Drug Eruption (FDE): Changing scenario of incriminating drugs. Int J Dermatol 2006;45:897-908.
[Google Scholar]
|
| 108. |
Smoller BR, Luster AD, Krane JF, Krueger J, Gray MH, McNutt NS, et al. Fixed drug eruptions: Evidence for a cytokine-mediated process. J Cutan Pathol 1991;18:13-9.
[Google Scholar]
|
| 109. |
Hindsen M, Christensen OB, Gruic V, Löfberg H. Fixed drug eruption: An immunohistochemical investigation of the acute and healing phase. Br J Dermatol 1987;116:351-60.
[Google Scholar]
|
| 110. |
Van Voorhees A, Stenn KS. Histological phases of bactrim-induced fixed drug eruption. The report of one case. Am J Dermatopathol 1987;9:528-32.
[Google Scholar]
|
| 111. |
Bedi TR, Pinkus H. Histopathological spectrum of erythema multiforme. Br J Dermatol 1976;95:243-50.
[Google Scholar]
|
| 112. |
Solomon AR Jr. The histologic spectrum of the reactive inflammatory vesicular dermatoses. Dermatol Clin 1985;3:171-83.
[Google Scholar]
|
| 113. |
Ackerman AB, Ragaz A. Erythema multiforme. Am J Dermatopathol 1985;7:133-9.
[Google Scholar]
|
| 114. |
Parsons JM. Toxic epidermal necrolysis. Int J Dermatol 1992;31:749-68.
[Google Scholar]
|
| 115. |
Stone N, Sheerin S, Burge S. Toxic epidermal necrolysis and graft vs. host disease: A clinical spectrum but a diagnostic dilemma. Clin Exp Dermatol 1999;24:260-2.
[Google Scholar]
|
| 116. |
Akosa AB, Elhag AM. Toxic epidermal necrolysis. A study of the sweat glands. J Cutan Pathol 1995;22:359-64.
[Google Scholar]
|
| 117. |
Sehgal VN, Srivastava G. Toxic epidermal necrolysis (TEN) Lyell's syndrome. J Dermatolog Treat 2005;16:278-86.
[Google Scholar]
|
| 118. |
Berger TG, Dhar A. Lichenoid photoeruptions in human immunodeficiency virus infection. Arch Dermatol 1994;130:609-13.
[Google Scholar]
|
| 119. |
Rico MJ, Kory WP, Gould EW, Penneys NS. Interface dermatitis in patients with the acquired immunodeficiency syndrome. J Am Acad Dermatol 1987;16:1209-18.
[Google Scholar]
|
| 120. |
Horn TD, Zahurak ML, Atkins D, Solomon AR, Vogelsang GB. Lichen planus-like histopathologic characteristics in the cutaneous graft-vs-host reaction. Prognostic significance independent of time course after allogeneic bone marrow transplantation. Arch Dermatol 1997;133:961-5.
[Google Scholar]
|
| 121. |
Saijo S, Honda M, Sasahara Y, Konno T, Tagami H. Columnar epidermal necrosis: A unique manifestation of transfusion-associated cutaneous graft-vs-host disease. Arch Dermatol 2000;136:743-6.
[Google Scholar]
|
| 122. |
Saurat JH, Gluckman E, Bussel A, Didierjean L, Puissant A. The lichen planus-like eruption after bone marrow transplantation. Br J Dermatol 1975;93:675-81.
[Google Scholar]
|
| 123. |
Pittelkow MR, Daud MZ. Lichen Planus. In: Wolff K, Gold Smith LA, Katz SI, et al, editors. Fitzpatrick's Dermatology in Genneral Medicine. 7 th ed. New York: Mc Graw Hill Medical; 2008. p 244-55.
th ed. New York: Mc Graw Hill Medical; 2008. p 244-55.'>[Google Scholar]
|
| 124. |
Sehgal VN, Srivastava G. Paraneoplastic pemphigus/paraneoplastic autoimmune multiorgan syndrome. Int J Dermatol 2009;48:162-9.
[Google Scholar]
|
| 125. |
Clark WH, Reed RJ, Mihm MC. Lupus erythematosus. Histopathology of cutaneous lesions. Hum Pathol 1973;4:157-63.
[Google Scholar]
|
| 126. |
Winkelmann RK. Spectrum of lupus erythematosus. J Cutan Pathol 1979;6:457-62.
[Google Scholar]
|
| 127. |
Jacobs MI, Schned ES, Bystryn JC. Variability of the lupus band test. Results in 18 patients with systemic lupus erythematosus. Arch Dermatol 1983;119:883-9.
[Google Scholar]
|
| 128. |
Monroe EW. Lupus band test. Arch Dermatol 1977;113:830-4.
[Google Scholar]
|
| 129. |
Bangert JL, Freeman RG, Sontheimer RD, Gilliam JN. Subacute cutaneous lupus erythematosus and discoid lupus erythematosus. Comparative histopathologic findings. Arch Dermatol 1984;120:332-7.
[Google Scholar]
|
| 130. |
Jerdan MS, Hood AF, Moore GW, Callen JP. Histopathologic comparison of the subsets of lupus erythematosus. Arch Dermatol 1990;126:52-5.
[Google Scholar]
|
| 131. |
Bielsa I, Herrero C, Collado A, Cobos A, Palou J, Mascaró JM. Histopathologic findings in cutaneous lupus erythematosus. Arch Dermatol 1994;130:54-8.
[Google Scholar]
|
| 132. |
Stefanato CM, Goldberg LJ, Andersen WK, Bhawan J. Gianotti-Crosti syndrome presenting as lichenoid dermatitis. Am J Dermatopathol 2000;22:162-5.
[Google Scholar]
|
| 133. |
Nikkels AF, Sadzot-Delvaux C, Rentier B, Piérard-Franchimont C, Piérard GE. Low-productive alpha-herpesviridae infection in chronic lichenoid dermatoses. Dermatology 1998;196:442-6.
[Google Scholar]
|
| 134. |
Suarez J, Lopez B, Villaba R, Perera A. Febrile ulceronecrotic Mucha-Habermann disease: A case report and review of the literature. Dermatology 1996;192:277-9.
[Google Scholar]
|
| 135. |
Katoulis AC, Stavrianeas NG, Georgala S, Katsarou-Katsari A, Koumantaki-Mathioudaki E, Antoniou C, et al. Familial cases of poikiloderma of civatte: Genetic implications in its pathogenesis? Clin Exp Dermatol 1999;24:385-7.
[Google Scholar]
|
| 136. |
Person JR, Bishop GF. Is poikiloderma a graft-versus-host-like reaction? Am J Dermatopathol 1984;6:71-2.
[Google Scholar]
|
| 137. |
Janis JF, Winkelmann RK. Histopathology of the skin in dermatomyositis. A histopathologic study of 55 cases. Arch Dermatol 1968;97:640-50.
[Google Scholar]
|
| 138. |
Ito A, Funasaka Y, Shimoura A, Horikawa T, Ichihashi M. Dermatomyositis associated with diffuse dermal neutrophilia. Int J Dermatol 1995;34:797-8.
[Google Scholar]
|
| 139. |
Chen Z, Maize JC, Silver RM, Dobson RL, Maricq HR, Ainsworth SK. Direct and indirect immunofluorescent findings in dermatomyositis. J Cutan Pathol 1985;12:18-27.
[Google Scholar]
|
| 140. |
Wang WJ. Clinical features of cutaneous amyloidoses. Clin Dermatol 1990;8:13-9.
[Google Scholar]
|
| 141. |
Horn TD, Redd JV, Karp JE, Beschorner WE, Burke PJ, Hood AF. Cutaneous eruptions of lymphocyte recovery. Arch Dermatol 1989;125:1512-7.
[Google Scholar]
|
| 142. |
Horn TD. Acute cutaneous eruptions after marrow ablation: Roses by other name? J Cutan Pathol 1994;21:385-92.
[Google Scholar]
|
| 143. |
Waisman M, Waisman M. Lichen aureus. Arch Dermatol 1976;112:696-7.
[Google Scholar]
|
| 144. |
Sardana K, Sarkar R, Sehgal VN. Pigmented purpuric dermatoses (PPD): An overview. Int J Dermatol 2004;43:482-8.
[Google Scholar]
|
| 145. |
Friedman SJ. Lichen spinulosus. Clinicopathologic review of thirty-five cases. J Am Acad Dermatol 1990;22:261-4.
[Google Scholar]
|
Fulltext Views
54,844
PDF downloads
6,012





![[Table - 1]](#tbl_ijdvl_2011_77_4_418_82389_t1.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2011_77_4_418_82389_f4.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_4_418_82389_f5.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_4_418_82389_f6.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2011_77_4_418_82389_f7.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2011_77_4_418_82389_t2.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2011_77_4_418_82389_t3.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2011_77_4_418_82389_f8.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2011_77_4_418_82389_f9.jpg){kind=link}
![[Figure - 7]](#fig_ijdvl_2011_77_4_418_82389_f10.jpg){kind=link}
![[Figure - 8]](#fig_ijdvl_2011_77_4_418_82389_f11.jpg){kind=link}
![[Figure - 9]](#fig_ijdvl_2011_77_4_418_82389_f12.jpg){kind=link}