Translate this page into:
Cutaneous metastasis of the small cell lung cancer
2 Department of Dermatology, Yuzuncuyil University Hospital, Van, Turkey
3 Department of Plastic and Reconstructive Surgery, Kecioren Research and Training Hospital, Ankara, Turkey
Correspondence Address:
Gulcin Guler Simsek
Department of Pathology, Ankara Kecioren Research and Training Hospital, Ankara
Turkey
| How to cite this article: Simsek GG, Karadag AS, Turksen Z. Cutaneous metastasis of the small cell lung cancer. Indian J Dermatol Venereol Leprol 2011;77:537 |
Sir,
Cutaneous metastases of the different visceral malignancies (0.7-9%) [1],[2] and also skin metastases of the lung cancer are rare, but worsen the prognosis (1-12%). [3],[4],[5]
While skin metastasis rate of large cell lung carcinomas is high, it is low for the squamous and small cell lung carcinomas. In this letter, we present a case of small cell lung carcinoma presenting with a cutaneous metastasis.
A 59-year-old male patient with the diagnosis of small cell lung carcinoma was referred to our clinic with the complaint of a painless, hard, and lumpy nodule on his left shoulder. He had history of chronic obstructive pulmonary disease. A submucosal lesion was observed during the bronchoscopy of the left lower lung lobe 9 months ago. Microscopic examination of the bronchoscopic biopsy revealed the diagnosis of small cell lung carcinoma and he was given four sessions of chemotherapy (Etapocid and Cisplatine). Post-therapeutic abdominal ultrasonography showed no metastasis. Three months after the cancer diagnosis, a lump formed on his left shoulder and progressed slowly.
On dermatological examination, an indurated, erythematous, and hard nodular lesion was detected on his left shoulder. Its largest diameter was 3 cm [Figure - 1]. An excisional biopsy revealed that the tumor was filling all the dermis in a diffuse pattern. There was no relation or invasion to the epidermis above. Tumor cells had hyperchromatic nuclei and high nucleocytoplasmic ratio [Figure - 2]. The mitotic index was high. Immunohistochemically tumor cells expressed cytokeratin7 [Figure - 3], chromogranin, and synaptophysin [Figure - 4]. The cells were negative for cytokeratin 20 and melan-A. Histopathological diagnosis was metastatic small cell lung carcinoma. The patient refused chemotherapy and he died 6 months after the diagnosis of skin metastasis.
 |
| Figure 1: Indurated, erythematous, and hard nodular lesion on left shoulder |
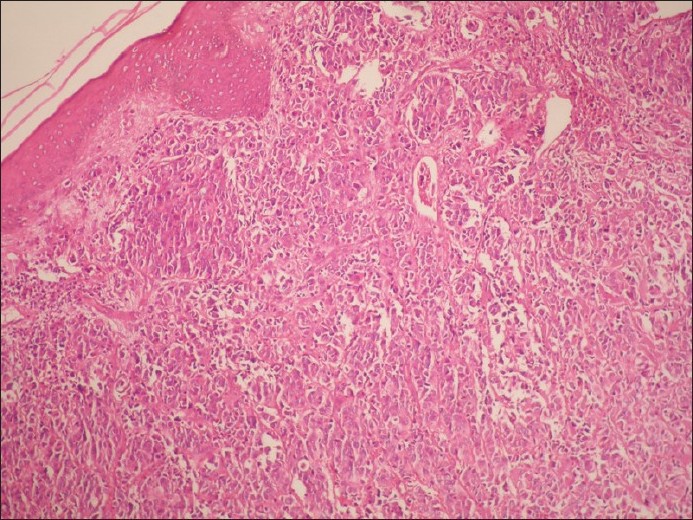 |
| Figure 2: Light microscopic image, diffusely distributed tumor in all of the dermis (H and E, ×100) |
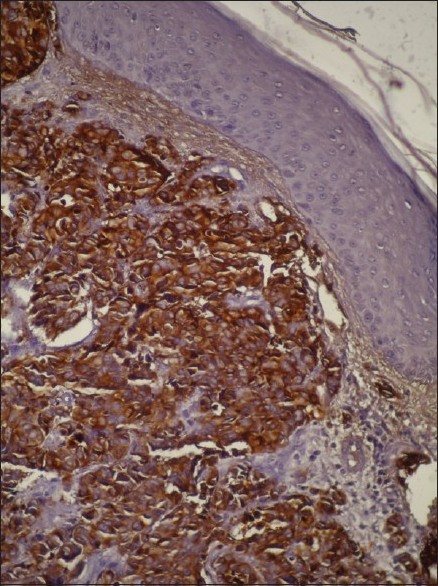 |
| Figure 3: Immunohistochemically tumor cells showing strong positivity with cytokeratin 7 (CK7, ×200) |
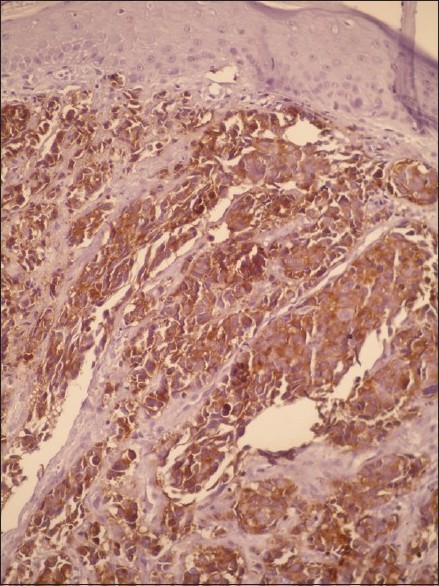 |
| Figure 4: Tumor cells expressing synaptophysin antigen (Synaptophysin, ×200) |
Skin manifestations of the patients with lung cancer were stated mostly as clubbing, cyanosis of lips, and telengiectasia. [3] Other symptoms of lung cancers include hypertrophic osteoarthropathy, acanthosis nigricans, edema, dermatomyositis, scleroderma, pachydermoperiostitis, and cervical lymphadenitis. [3] Patients diagnosed with lung carcinoma are at a substantial risk of metastasis. Even when the disease is detected at an early stage and removed by surgery, relapse with widespread metastases can be rapid. The most likely metastatic route is the hematogenous spread. The basic metastatic course can occur in the following steps: detachment from the primary tumor followed by invasion, intravasation into a vessel, circulation, stasis within a vessel, extravasation, invasion into recipient tissue bed, and proliferation. [2]
Skin metastases of the lung cancer are rare and worsen the prognosis. The rate of the cutaneous metastases changes according to the types. It was found as 0.81% for small cell lung carcinomas. It is much lower compared to adenocarcinomas (2.95%) and squamous cell carcinomas (1.16%) of the lung. Clinical findings include a red-pink, ulcerated nodule and skin metastasis may be the first sign of the tumor. [3],[5] Therefore, it is important for both dermatologists and pathologists to be able recognize and diagnose these metastases.
Although they can occur in any part of the skin, most common sites for cutaneous metastases are chest, back, abdomen, and scalp. [5] Our patient′s cancer was located on left lower pole of the lung, and skin metastasis developed on his left shoulder. Skin metastasis worsens the prognosis of the patients. By the time skin metastasis appear, the neoplasm has usually advanced far. Median survival time after the diagnosis of a cutaneous metastasis is between 2.9 and 4.9 months. [5] Treatment modalities cannot usually change this progress. Our patient died 6 months after the diagnosis of the cutaneous metastasis.
As seen in this case of rare unexpected skin metastasis of small cell lung carcinoma, the skin metastases lack a pathognomonic physical appearance. Therefore, physicians should be vigilant about this entity. Atypical skin lesions of the cancer patients, even they are not on common sites, should be evaluated and biopsies should be done to diagnose metastases and consider further adjuvant and supportive treatments.
| 1. |
Hu SC, Chen GS, Lu YW, Wu CS, Lan CC. Cutaneous metastases from different internal malignancies: A clinical and prognostic appraisal. J Eur Acad Dermatol Venereol 2008;22:735-40.
[Google Scholar]
|
| 2. |
Rosen T. Cutaneous metastases. Med Clin North Am 1980;64:885-900.
[Google Scholar]
|
| 3. |
Kökçam Ý, Yavrucuoðlu E, Saral Y, Muz H, Çelik P. Skin manifestations of the patients with lung cancer. Turk J Dermatol 1994;3:156-9.
[Google Scholar]
|
| 4. |
Barbetakis N, Samanidis G, Paliouras D, Samanidou E, Tzimorota Z, Asteriou C, et al. Facial skin metastasis due to small-cell lung cancer: A case report. J Med Case Reports 2009;3:32.
[Google Scholar]
|
| 5. |
Hürmüz P, Selek U, Zorlu F, Tekuzman G. Lung adenocarcinoma with skin metastasis. Int J Hematol Oncol 2008;18:39-41.
[Google Scholar]
|
Fulltext Views
3,160
PDF downloads
1,863





![[Figure - 1]](#fig_ijdvl_2011_77_4_537_82430_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_4_537_82430_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_4_537_82430_u3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2011_77_4_537_82430_u4.jpg){kind=link}