Translate this page into:
Annular scaly plaques in a girl
Correspondence Address:
Swagata Arvind Tambe
19/558, Udyan Society, Nehru Nagar, Kurla East, Mumbai - 400 024, Maharashtra
India
| How to cite this article: Parulkar P, Tambe SA, Nayak CS. Annular scaly plaques in a girl. Indian J Dermatol Venereol Leprol 2020;86:98-100 |
A 13-year-old female, born of nonconsanguineous marriage presented with complaints of sudden onset of multiple red raised circular lesions on the trunk of 8 days duration associated with mild itching. There was no history of preceding upper respiratory tract infection, febrile illness or drug intake.
Cutaneous examination revealed multiple erythematous annular scaly plaques with central hyperpigmentation, and raised margins on the upper back [Figure - 1], upper chest [Figure - 2] and trunk [Figure - 3]. A single large plaque was also present on the right side of the neck extending to the shoulder. There was no evidence of regional or generalized lymphadenopathy.
 |
| Figure 1: Multiple erythematous annular scaly plaques with central hyperpigmentation and raised margins on upper back |
 |
| Figure 2: Erythematous annular scaly plaques on shoulders and chest |
 |
| Figure 3: Erythematous annular scaly plaques on the trunk |
Skin biopsy showed parakeratotic stratum corneum overlying severely spongiotic epidermis with upper dermal edema and superficial perivascular mixed inflammatory infiltrate consisting of mononuclear cells and neutrophils with extravasated red blood cells in the dermis [Figure - 4] and [Figure - 5].
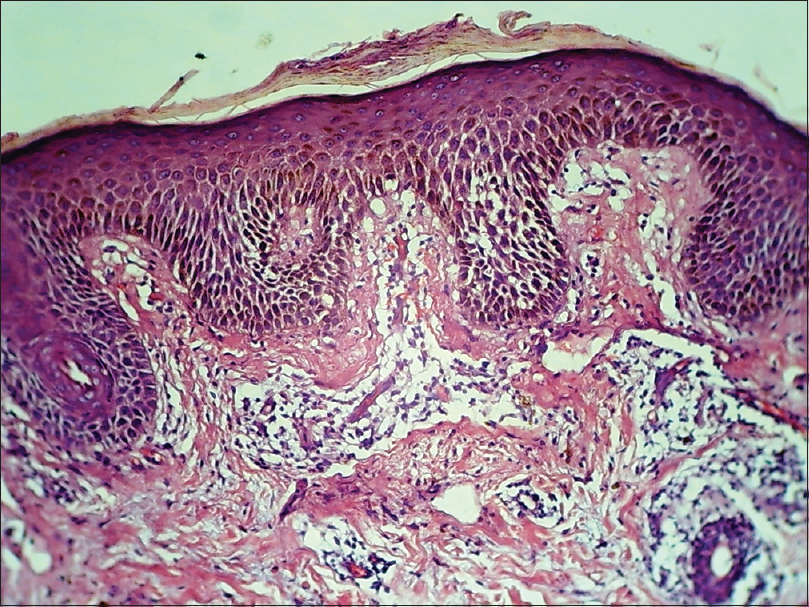 |
| Figure 4: Parakeratosis, spongiosis with upper dermal edema and superficial perivascular mixed inflammatory infiltrate in the dermis (H and E, ×100) |
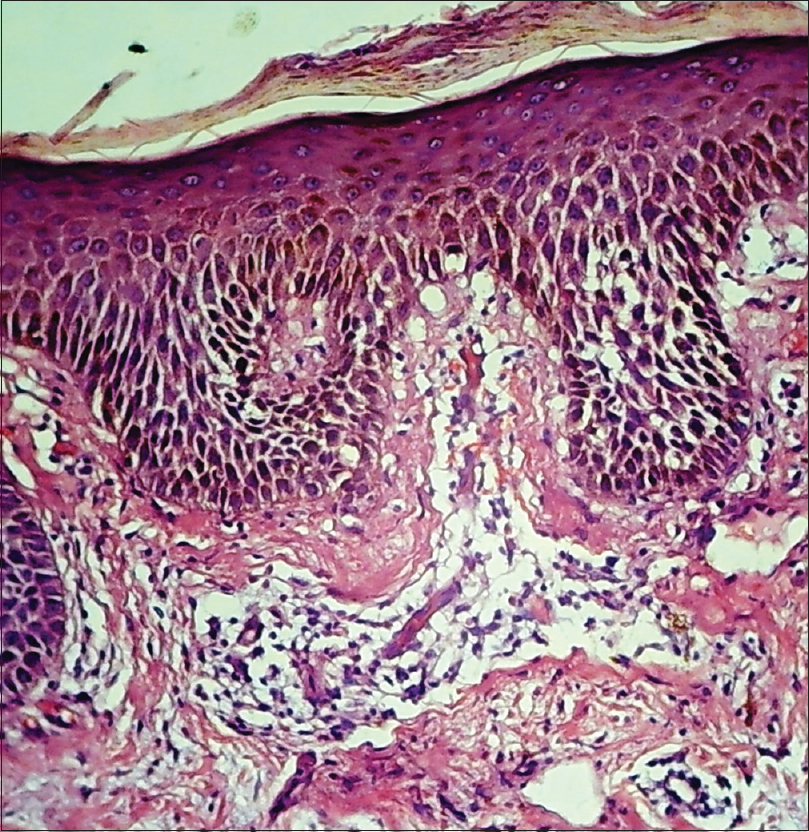 |
| Figure 5: Marked spongiosis, dermal edema and dilated blood vessels in dermis with extravasated red blood cells (H and E, ×400) |
Laboratory investigations including enzyme-linked immunosorbent assay for human immunodeficiency virus (HIV) and Venereal Disease Research Laboratory test did not reveal any abnormality.
Answer
Pityriasis rosea.
Pityriasis rosea is an acute, common, self-limiting, papulosquamous disorder localized to the trunk and extremities of children and young adults. It is characterized by the initial eruption of a herald patch (mother patch), which is followed by generalized scaly oval eruptions typically on the trunk and proximal extremities along the Langer's lines of cleavage, giving the characteristic “Christmas tree appearance”. Approximately 20% of patients with pityriasis rosea may present with atypical clinical presentations.[1],[2] Atypical features include atypical morphology of rash, size of lesions, number of lesions, distribution, mucosal involvement, symmetry, disease duration and severity of symptoms. Indian children are more likely to present with atypical pityriasis rosea than Indian adults, atopic background being possibly facilitative.[3] Although no etiology has been proven, viral agents, especially human herpes virus 6 and 7, autoimmunity, several drugs and psychogenic status have been proposed as possible etiological factors.[1],[2],[4]
Atypical variants can be differentiated by size (pityriasis rosea gigantea of Darier, papular pityriasis rosea), distribution (cephalic pityriasis rosea, inverse pityriasis rosea, unilateralis pityriasis rosea, localized pityriasis rosea and pityriasis circinata et marginata of Vidal), sites involved (face, scalp, hands and feet, fingers, toes, eyelids, penis and oral cavity), severity (pityriasis rosea irritata with severe itch, pain and a burning sensation), course of the lesions (relapse, recurrent pityriasis rosea, annual relapse) and morphology (generalized papular, vesicular, purpuric or hemorrhagic,[5] urticarial, pustular and erythema multiforme like pityriasis rosea).[1],[4],[6]
There have been several case reports in the literature describing the clinical features of variants of pityriasis rosea but plaques with prominent scaling and large annular morphology is not a commonly reported variant.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Chuh A, Zawar V, Lee A. Atypical presentations of pityriasis rosea: Case presentations. J Eur Acad Dermatol Venereol 2005;19:120-6.
[Google Scholar]
|
| 2. |
González LM, Allen R, Janniger CK, Schwartz RA. Pityriasis rosea: An important papulosquamous disorder. Int J Dermatol 2005;44:757-64.
[Google Scholar]
|
| 3. |
Zawar V, Chuh A. Follicular pityriasis rosea. A case report and a new classification of clinical variants of the disease. J Dermatol Case Rep 2012;6:36-9.
[Google Scholar]
|
| 4. |
Miranda SB, Lupi O, Lucas E. Vesicular pityriasis rosea: Response to erythromycin treatment. J Eur Acad Dermatol Venereol 2004;18:622-5.
[Google Scholar]
|
| 5. |
Bhalla N, Tambe S, Zawar V, Joshi R, Jerajani H. Localized purpuric lesions in a case of classical pityriasis rosea. Indian J Dermatol Venereol Leprol 2014;80:551-3.
[Google Scholar]
|
| 6. |
Balci DD, Hakverdi S. Vesicular pityriasis rosea: An atypical presentation. Dermatol Online J 2008;14:6.
[Google Scholar]
|
Fulltext Views
5,719
PDF downloads
3,514





![[Figure - 1]](#fig_ijdvl_2020_86_1_98_235645_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_1_98_235645_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2020_86_1_98_235645_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2020_86_1_98_235645_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2020_86_1_98_235645_f5.jpg){kind=link}