Translate this page into:
A solitary nodule on the posterior pinna
Correspondence Address:
Hoon Kang
Department of Dermatology, St. Paul's Hospital, College of Medicine, The Catholic University of Korea, 180, Wangsan-ro, Dongdaemun-gu, Seoul 02559
Korea
| How to cite this article: Sohn KM, Woo YJ, Kim JE, Kang H. A solitary nodule on the posterior pinna. Indian J Dermatol Venereol Leprol 2019;85:111-113 |
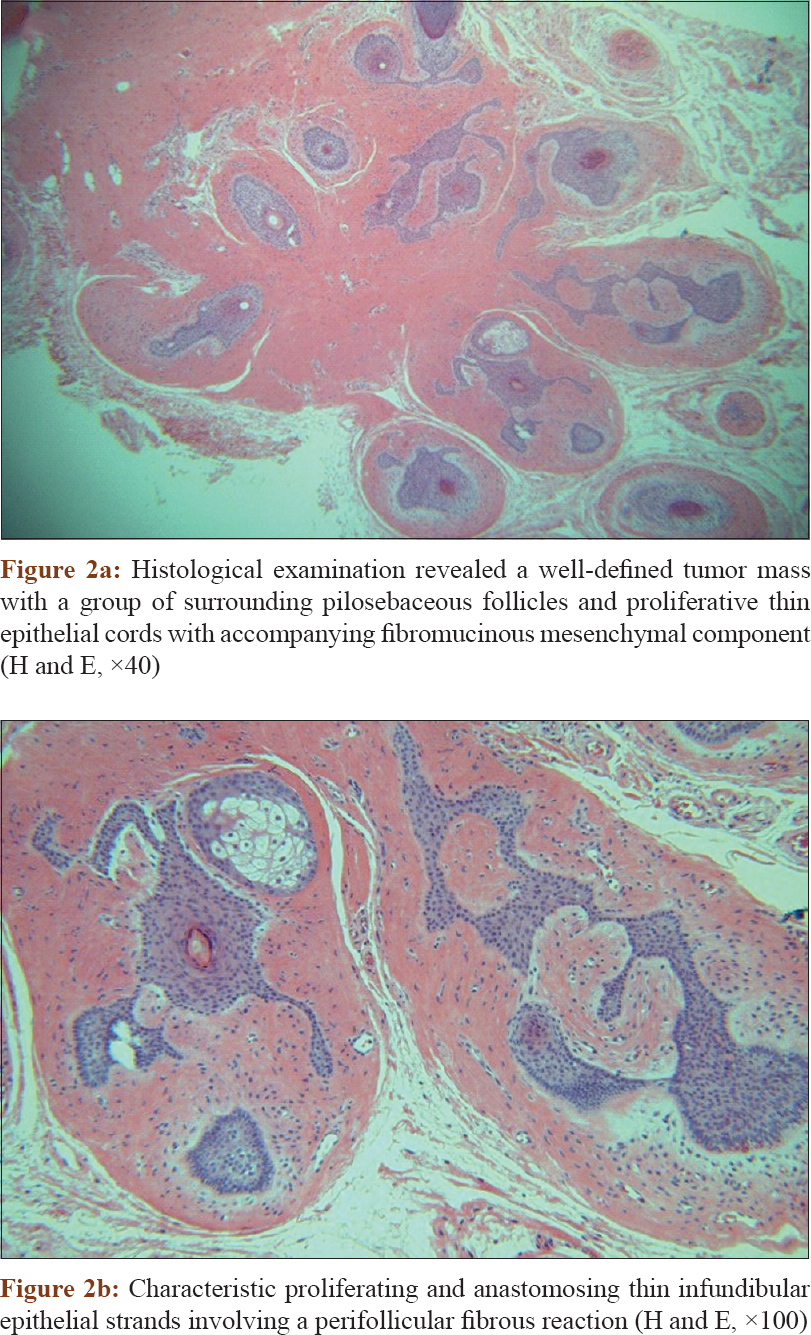
A 50-year-old man presented with a solitary, slightly pruritic, flesh-colored, 1.0 × 1.2 cm-sized nodule on the right posterior auricular area that had been noticeable for 3 years [Figure - 1]. He had a habit of scratching and rubbing the lesion frequently. His past medical and family histories were unremarkable. Physical examination revealed a mildly lichenified patch around the nodule, and no other remarkable cutaneous features were observed. A shave biopsy was performed. Histological examination showed a well-defined tumor mass with a group of surrounding pilosebaceous follicles and proliferative thin epithelial cords, accompanied by fibromucinous mesenchymal components. In addition, characteristic proliferating and anastomosing thin infundibular epithelial strands with a perifollicular fibrous reaction were seen [Figure - 2].
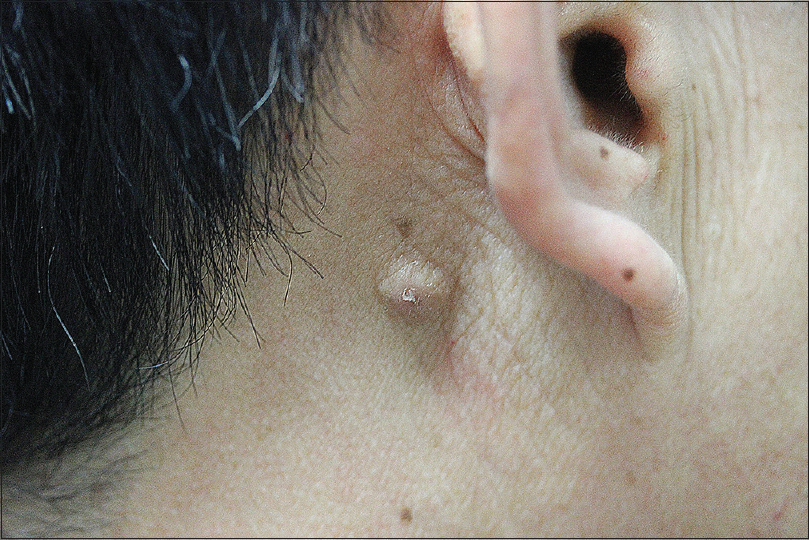 |
| Figure 1: A slightly pruritic, solitary, firm, flesh-colored, 1.0 cm × 1.2 cm-sized nodule with central punctum and peripheral mild lichenification on the posterior auricular area |
 |
| Figure 2: |
What is Your Diagnosis?
Answer
Fibrofolliculoma
Review
Fibrofolliculomas are benign perifollicular connective tissue tumors which are often multiple and inherited as an autosomal dominant trait.[1] Although most cases of multiple fibrofolliculomas have been reported in association with other clinical findings, such as Birt–Hogg–Dubé syndrome [caused by germline mutations of the folliculin (FLCN) gene, and characterized by skin lesions (trichodiscomas, perifollicular fibromas and acrochordons) and systemic associations (pulmonary cysts and renal tumors)], sporadic cases without associated clinical findings have also been reported.[1],[2],[3]
Clinically, fibrofolliculomas present with asymptomatic, 2–4 mm, flesh-colored, dome-shaped smooth papules. They usually arise in adults in areas with abundant hair follicles, such as the scalp and face.[1] The first case was described by Birt et al.[4] in 1977, and most subsequently reported cases had multiple lesions. Solitary fibrofolliculoma is a very rare presentation.[1],[2],[3],[5]
Although solitary fibrofolliculoma occurs infrequently, its clinical and histological features are identical to those of multiple fibrofolliculomas except the lack of association with other cutaneous lesions.[2] To our knowledge, only six reports, involving ten cases of solitary fibrofolliculoma, have been noted in relevant literature.[1],[2],[3],[5] With the exception of one case of Birt–Hogg–Dubé syndrome presenting with a single pedunculated fibrofolliculoma on the nose,[5] other cases occurred sporadically on the scalp, face, and concha of the ear.
Due to its tendency to appear on skin with abundant hair follicles, fibrofolliculoma is expected to occur more readily on the scalp and face. The posterior auricular area is a location that has comparatively fewer hair follicles than the scalp and face. The lichenification around the mass may suggest that minor trauma by scratching may be the possible etiology in our particular case.
The clinical differential diagnosis of fibrofolliculoma includes epidermoid cysts, trichofolliculoma, angiofibroma, basal cell carcinoma, acrochordon, and trichoepitheliomas.[1] Histologically, fibrofolliculoma must be differentiated from other epithelial and mesodermal tumors of the hair, which include trichofolliculoma, perifollicular fibroma, trichoepithelioma, trichilemmoma, trichodiscoma, angiofibroma, and basaloid follicular hamartoma.[1],[2] Trichofolliculoma shows a large comedo-like lesion into which numerous small hair follicles with trichohyaline granules and vellus hairs open. Perifollicular fibroma exhibits perifollicular concentric accentuation of the fibrous tissue. Trichoepithelioma shows reticular-patterned basaloid tumor islands, commonly with horn cysts. Trichilemmoma shows hyperkeratosis with downward lobular epidermis, with thin rims of palisading basal cells. Trichodiscoma exhibits fine fibrillary connective tissue containing ectatic blood vessels in the dermis. Angiofibroma shows a fine vascular proliferation with associated fibrosis in the dermis. Basaloid follicular hamartoma shows vertically oriented basaloid cells centered upon a comedo-like follicle.
For the treatment of solitary fibrofolliculoma, multiple ablative therapies including excision, dermabrasion, laser therapy, and electrodesiccation can be done, though additional screening for other cutaneous or extracutaneous features is needed.
We report a rare case of fibrofolliculoma that occurred on the posterior auricular area, which is an unusual location for fibrofolliculoma. Despite its rare occurrence, dermatologists should bear in mind the consideration of a diagnosis of solitary fibrofolliculoma when a similar skin lesion is observed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Starink TM, Brownstein MH. Fibrofolliculoma: solitary and multiple types. J Am Acad Dermatol 1987;17:493-6.
[Google Scholar]
|
| 2. |
Cho E, Lee JD, Cho SH. A solitary fibrofolliculoma on the concha of the ear. Int J Dermatol 2012;51:616-7.
[Google Scholar]
|
| 3. |
Chang JK, Lee DC, Chang MH. A solitary fibrofolliculoma in the eyelid. Korean J Ophthalmol 2007;21:169-71.
[Google Scholar]
|
| 4. |
Birt AR, Hogg GR, Dubé WJ. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatol 1977;113:1674-7.
[Google Scholar]
|
| 5. |
César A, Baudrier T, Mota A, Azevedo F. A case of Birt-Hogg-Dubé syndrome presenting with a single pedunculated fibrofolliculoma and a novel FLCN gene mutation. Actas Dermosifiliogr 2016;107:541-3.
[Google Scholar]
|
Fulltext Views
3,275
PDF downloads
2,820





![[Figure - 1]](#fig_ijdvl_2019_85_1_111_223999_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2019_85_1_111_223999_f2.jpg){kind=link}