Translate this page into:
Angioma like carcinoma telangiectoides: An unusual presentation of breast carcinoma metastasis
2 Department of Pathology, All India Institute of Medical Sciences, New Delhi, India
Correspondence Address:
Sujay Khandpur
Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi - 110 029
India
| How to cite this article: Patra S, Khandpur S, Khanna N, Jain D. Angioma like carcinoma telangiectoides: An unusual presentation of breast carcinoma metastasis. Indian J Dermatol Venereol Leprol 2018;84:83-85 |
Sir,
Breast carcinoma is the most common tumor associated with cutaneous metastasis in women. Cutaneous involvement can occur by direct invasion, local spread through dermal vessels or as distant metastasis. Morphologically, metastasis can present with various clinical and histopathological patterns. We report a patient who presented with telangiectatic carcinoma with angioma-like papules on the breast and anterior chest wall. This case is being reported to depict uncommon morphology of cutaneous breast carcinoma metastasis.
A 51-year-old woman was diagnosed with carcinoma of the left breast, stage T4N1M1, with metastasis to the opposite breast and skeletal metastasis involving the lumbosacral vertebrae. It was infiltrative lobular carcinoma grade 2, estrogen receptor (ER) negative, progesterone receptor (PR) negative and HER 2 positive. She was on palliative chemotherapy. Initially, she received 6 cycles of epirubicin and docetaxel along with localized radiotherapy for skeletal metastasis, followed by 6 cycles of paclitaxel + herceptin and 6 cycles of herceptin + vinorebiline due to initial relapse after 2 months. Positron emission tomography (PET) scan done after the last regimen change showed response to therapy. Subsequently within the next 2 months, she presented with erythema and itching over both breasts associated with erythematous papules gradually extending in size. On examination, there was partially blanchable erythema over the right breast and adjoining part of the left breast including the upper anterior portion of the chest wall [Figure - 1]. Overlying the erythema, there were multiple, 1–2-mm sized erythematous nonblanchable, firm, angiomatous papules [Figure - 2]. There was no skin induration and no increase in surface temperature but an ill-defined mass could be palpated in the right breast. There was no regional lymphadenopathy. A skin biopsy obtained from one of the red-colored papules revealed a normal epidermis, and in the upper dermis, there were multiple dilated capillaries containing intravascular metastatic deposits of tumor cells [Figure - 3]. The tumor cells were ER and PR negative [Figure - 4], and HER 2 positive [Figure - 5], similar to the primary breast tumor. CD34 staining highlighted endothelial cells indicating the intravascular location of the metastatic deposits [Figure - 6]. A diagnosis of carcinoma telangiectoides mimicking angiomas was made. A repeat PET scan done a month after the detection of cutaneous metastasis showed active residual disease in the right breast, left axillary lymph nodes and the right humerus. This prompted the oncologists to change her chemotherapy to capecitabine and lapatinib to which also she responded poorly.
 |
| Figure 1: Background erythema of the skin with overlying dusky erythematous papules |
 |
| Figure 2: Multiple angioma-like papules |
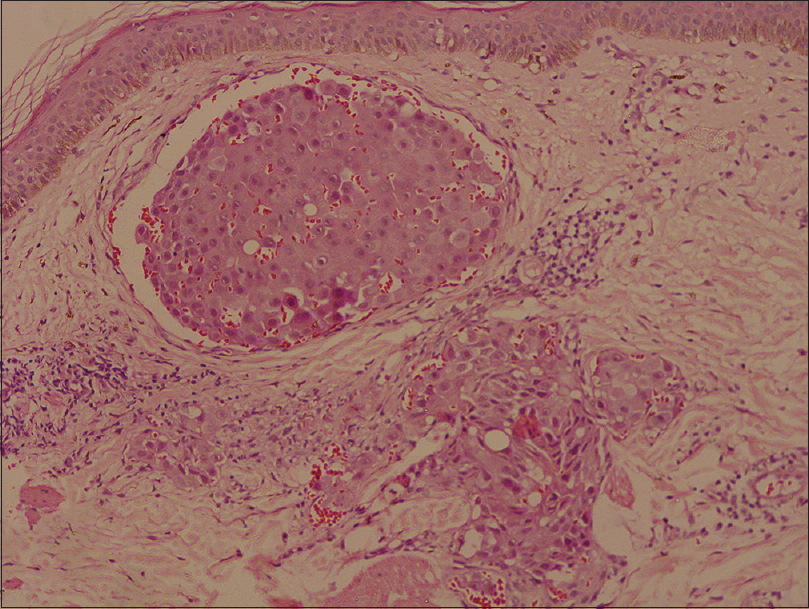 |
| Figure 3: Dilated blood vessels in upper dermis with intravascular tumor cells (H and E, ×400) |
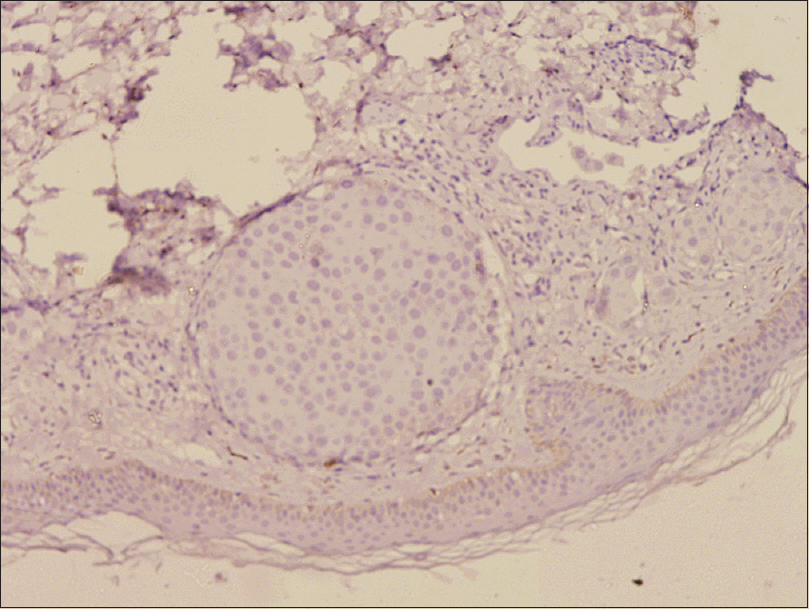 |
| Figure 4: Tumor cells are negative for estrogen receptor and progesterone receptor |
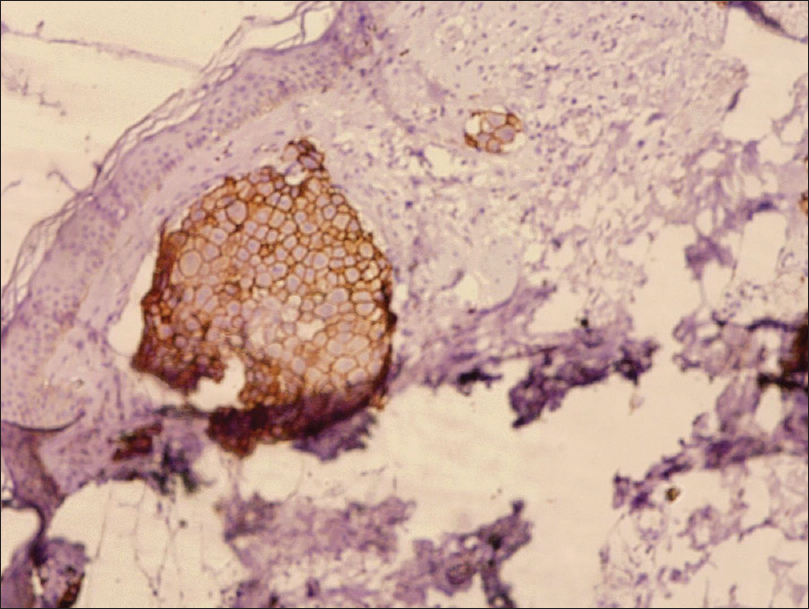 |
| Figure 5: Special stains with human epidermal growth factor receptor 2 showed positivity in tumor cells |
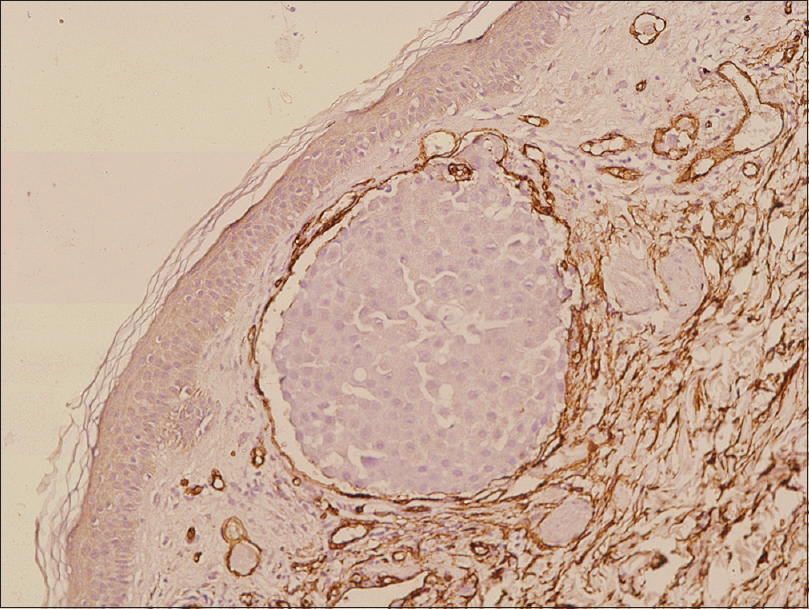 |
| Figure 6: CD34 staining for endothelial cells showed intravascular location of tumor cells |
Cutaneous metastasis comprises 2% of all skin malignancies and occurs in 0.6–10.4% of the patients with internal malignancies.[1] In a series of 164 cases by Mordenti et al., it was shown that cutaneous metastasis from breast carcinoma could manifest as papules and nodules (80%), telangiectatic carcinoma (11.2%), erysipeloid carcinoma (3%), “en cuirasse” carcinoma (3%), alopecia neoplastica (2%) or in zosteriform distribution (0.8%). Erysipeloides carcinoma usually presents as an erythematous, warm, tender plaque on the breast. Telangiectatic carcinoma manifests with papulovesicles, appearing on an erythematous telangiectatic surface, and histologically tumor dissemination is limited to the superficial lymphatics and blood vessels.[2],[3] Apart from breast carcinoma, carcinoma of parotid and uterus can also present as telangiectatic carcinoma.[4],[5] Although presence of papules of variable size and nodules have been noted in earlier case reports, angioma-like red tiny papules, as seen in our case, has not been reported. Other features in our case such as background erythema and absence of induration resembles the telangiectatic carcinoma subtype of cutaneous metastasis. This was confirmed by the presence of tumor cells within the lumen of cutaneous capillaries. Skin metastasis is usually associated with advanced stage of cancer and prognosis depends on the type and biological behavior of the underlying malignancy. The 5-year survival rate reported in cases with skin metastasis is less than 10%, which can be improved to up to 30–35% with a multimodality approach.[6] Difference in prognosis according to different types of cutaneous metastasis is not known. Our patient received several combination chemotherapy regimens to which she had poor response.
Acknowledgement
Geetika Srivastava MD, Department of Dermatology and Venereology, AIIMS, New Delhi.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Alcaraz I, Cerroni L, Rütten A, Kutzner H, Requena L. Cutaneous metastases from internal malignancies: A clinicopathologic and immunohistochemical review. Am J Dermatopathol 2012;34:347-93.
[Google Scholar]
|
| 2. |
Mordenti C, Peris K, Fargnoli MC, Cerroni L, Chimenti S. Cutaneous metastatic breast carcinoma: A study of 164 patients. Acta Dermatovenerol 2000;9:143-8.
[Google Scholar]
|
| 3. |
Lookingbill DP, Spangler N, Helm KF. Cutaneous metastases in patients with metastatic carcinoma: A retrospective study of 4020 patients. J Am Acad Dermatol 1993;29:228-36.
[Google Scholar]
|
| 4. |
Zanca A, Ferracini U, Bertazzoni MG. Telangiectatic metastasis from ductal carcinoma of the parotid gland. J Am Acad Dermatol 1993;28:113-4.
[Google Scholar]
|
| 5. |
Schwartz RA. Histopathologic aspects of cutaneous metastatic disease. J Am Acad Dermatol 1995;33:649-57.
[Google Scholar]
|
| 6. |
Jaiyesimi IA, Buzdar AU, Hortobagyi G. Inflammatory breast cancer: A review. J Clin Oncol 1992;10:1014-24.
[Google Scholar]
|
Fulltext Views
4,873
PDF downloads
2,281





![[Figure - 1]](#fig_ijdvl_2018_84_1_83_221311_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_1_83_221311_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2018_84_1_83_221311_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2018_84_1_83_221311_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2018_84_1_83_221311_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2018_84_1_83_221311_f6.jpg){kind=link}