Translate this page into:
Permanent treatment of aquagenic syringeal acrokeratoderma with endoscopic thoracic sympathectomy
2 Department of Pathology, Acıbadem University, School of Medicine, Istanbul, Turkey
Correspondence Address:
Engin Sezer
Department of Dermatology, Acibadem University, School of Medicine, Buyukdere Cad. No: 40, Maslak, Istanbul
Turkey
| How to cite this article: Sezer E, Durmaz E�, �etin E, Sahin S. Permanent treatment of aquagenic syringeal acrokeratoderma with endoscopic thoracic sympathectomy. Indian J Dermatol Venereol Leprol 2015;81:648-650 |
Sir,
A 31-year-old man was referred from the pulmonary surgery department for evaluation of palmar lesions which became prominent upon exposure to water, with a proposed treatment plan of endoscopic thoracic sympathectomy for his palmar hyperhidrosis. The patient had decided to undergo this procedure, despite its potential side effects, since his problem was refractory to topical aluminum chloride hexahydrate and tap water iontophoresis. Physical examination revealed whitish papules and dilated pores, with accentuation over palmar creases on both hands, together with tiny, translucent, punctate hyperkeratotic papules on the thenar surface and thumb of the right hand [Figure - 1]a. A water-immersion test (2 min of exposure to warm water) resulted in marked prominence of the lesions [Figure - 1]b. Punch biopsy specimens were obtained from a papule over the right palmar crease and a punctate lesion on the thenar prominence.
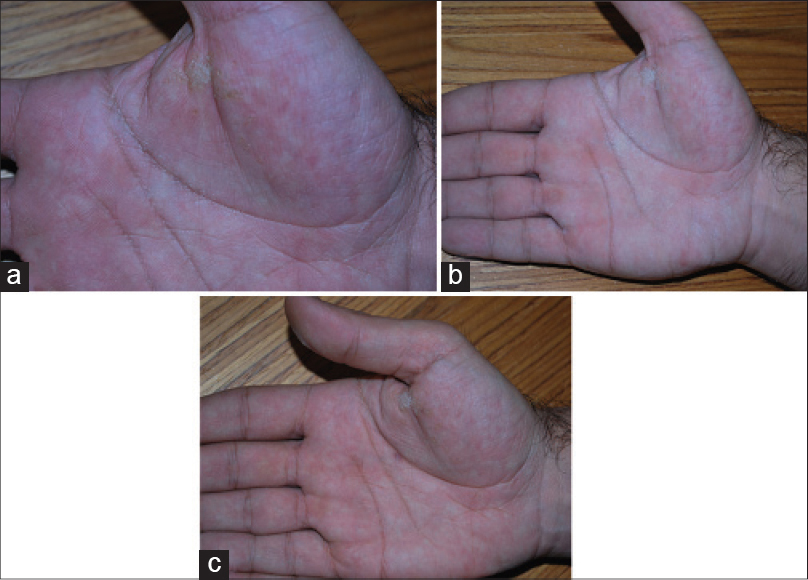 |
| Figure 1: (a) Whitish, translucent papules and dilated pores over the palmar creases. Punctate, hyperkeratotic lesions are alsoidentified on the thenar region of the palm. (b) A water immersiontest resulted in accentuation of the lesions. (c) After endoscopicthoracic sympathectomy, lesions on the palmar creases resolved while the thenar hyperkeratotic lesions persisted (clinical image was obtained after water immersion test) |
Histopathological examination of the biopsy specimen from the palmar crease revealed a dilated and tortuous acrosyringium with compact orthokeratosis [Figure - 2]a. Dermal inflammation was not identified. The second biopsy specimen from the thenar region revealed orthokeratosis without significant epidermal changes or altered acrosyringium [Figure - 2]b. A diagnosis of aquagenic syringeal acrokeratoderma on the palmar creases and punctate palmar keratoderma on the thenar surfaces was established, two distinct histopathological entities were thus observed in close proximity.
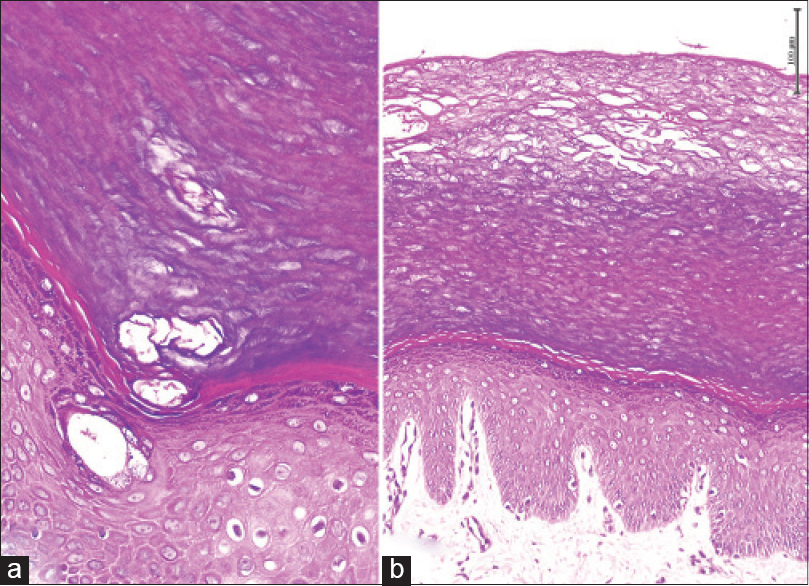 |
| Figure 2: (a) Biopsy from aquagenic syringeal acrokeratosis revealed dilated and tortuous acrosyringium with compact hyperkeratosis (Hematoxylin and Eosin, ×100). (b) Compact hyperkeratosis alone was identified in punctate keratoderma lesions (Hematoxylin and Eosin, ×40) |
An acquired sweat gland abnormality has been considered in the etiopathogenesis of aquagenic syringeal acrokeratoderma.[1] Since endoscopic thoracic sympathectomy is an effective treatment for suppression of eccrine gland function, the patient was informed about the potential benefits of this treatment modality and he decided to go ahead with this intervention. At 1 month follow-up after the procedure, there was complete resolution of the lesions on the palmar creases, but the thenar lesions persisted. Interestingly, the whitish papular lesions consistent with aquagenic syringeal acrokeratoderma did not reappear even after the water immersion test [Figure - 1]c. In contrast, no changes were observed in the punctate palmar keratoderma lesions on the thenar region. Topical 5% salicylic acid ointment initiated for these lesions which showed partial regression with treatment. No recurrence of aquagenic syringeal acrokeratoderma lesions were detected in a 1 year follow-up.
Aquagenic syringeal acrokeratoderma (synonyms: aquagenic palmoplantantar keratoderma, aquagenic wrinkling of the palms, transient reactive papulotranslucent keratoderma) is a rare disease of the palms and sometimes soles characterized by symmetrical, white or translucent papules or plaques which are accentuated following exposure to water. The etiopathogenesis of aquagenic syringeal acrokeratoderma is unclear. Frequent association with cystic fibrosis and a history of medication with cyclo-oxygenase (COX)-2 inhibitors in a subset of patients suggest that it is related to increased salt content in the skin.[2] Abnormal regulation of transmembrane channels such as aquaporin 3 and a role of weakness of eccrine duct walls have also been considered in its etiology. Although drugs such as celecoxib and rofecoxib have been reported to induce these lesions,[3] there was no such association in this case.
Palmar and/or plantar hyperhidrosis has been described in a subset of cases with aquagenic syringeal acrokeratoderma, as in this instance. Endoscopic thoracic sympathectomy is an effective and long-term treatment for palmar hyperhidrosis. Certain portions of the sympathetic nerve trunk are blocked with titanium clamps thereby inhibiting the catecholamine-containing nerve terminals of the eccrine sweat glands and reducing sweating. Improvement of the aquagenic syringeal acrokeratoderma lesions with sweat gland-suppressing treatment options such as botulinum toxin injection and topical aluminum chloride suggests aberration of eccrine sweat gland function as the etiopathogenesis of this rare entity. The disappearance of the whitish papular lesions in this case after endoscopic thoracic sympathectomy, even on long term follow up also supports this theory. We were unable to find any previous reports of the use of endoscopic thoracic sympathectomy as a permanent treatment approach for aquagenic syringeal acrokeratoderma. Other treatment modalities including topical aluminum chloride, 12% aluminum lactate cream, 3% formalin in alcohol, 5% salicylic acid ointment, petroleum-based barrier creams and botulinum toxin injection have all shown mixed and transient results.[4],[5]
An interesting feature in our patient was the persistence of punctate palmar keratoderma in spite of the resolution of papules of aquagenic syringeal acrokeratoderma papules. This strongly supports the notion that both of these entities are separate forms of keratoderma with the former representing an acquired sweat gland abnormality. We were unable to find any previous reports of this association, which also strengthens the view that aquagenic syringeal acrokeratoderma is part of the spectrum of palmar/plantar acrokeratodermas. Finally, we suggest that endoscopic thoracic sympathectomy may be considered to be a long-term treatment option for patients with aquagenic syringeal acrokeratoderma, especially if it is associated with severe palmar hyperhidrosis.
| 1. |
Luo DQ, Zhao YK, Zhang WJ, Wu LC. Aquagenic acrokeratoderma. Int J Dermatol 2010;49:526-31.
[Google Scholar]
|
| 2. |
Garçon-Michel N, Roguedas-Contios AM, Rault G, Le Bihan J, Ramel S, Revert K, et al. Frequency of aquagenic palmopantar keratoderma in cystic fibrosis: A new sign of cystic fibrosis? Br J Dermatol 2010;163:162-6.
[Google Scholar]
|
| 3. |
Tchernev G, Semkova K, Cardoso JC, Ananiev JJ, Wollina U. Aquagenic keratoderma. Two new case reports and a new hypothesis. Indian Dermatol Online J 2014;5:30-3.
[Google Scholar]
|
| 4. |
Diba VC, Cormack GC, Burrows NP. Botulinum toxin is helpful in aquagenic palmoplantar keratoderma. Br J Dermatol 2005;152:394-5.
[Google Scholar]
|
| 5. |
Erkek E. Unilateral transient reactive papulotranslucent acrokeratoderma in a child. Pediatr Dermatol 2007;24:564-6.
[Google Scholar]
|
Fulltext Views
5,645
PDF downloads
1,446





![[Figure - 1]](#fig_ijdvl_2015_81_6_648_168331_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_6_648_168331_f2.jpg){kind=link}