Translate this page into:
Pruritic porokeratotic peno-scrotal plaques: Porokeratosis or porokeratotic epidermal reaction pattern? A report of 10 cases
2 Mehta Clinic, Ratnagiri, Maharashtra, India
Correspondence Address:
Rajiv Joshi
14 Jay Mahal, A Road, Churchgate, Mumbai - 400 020, Maharashtra
India
| How to cite this article: Joshi R, Mehta SG. Pruritic porokeratotic peno-scrotal plaques: Porokeratosis or porokeratotic epidermal reaction pattern? A report of 10 cases. Indian J Dermatol Venereol Leprol 2014;80:24-28 |
Abstract
Background: Porokeratosis restricted to the genital region is rare with few cases described in the literature. Cases of porokeratosis restricted to the genital region are similar to plaque type of porokeratosis of Mibelli seen elsewhere on the body. We encountered 10 young males with pruritic plaques restricted to the peno-scrotal region, which clinically were not diagnosed as porokeratosis, but on biopsy revealed multiple cornoid lamellae, some of which were seen to arise from eccrine and follicular structures. Aims: The aim of this study is to study lesions restricted to the peno-scrotal region in males, which on biopsy showed cornoid lamellae suggestive of porokeratosis. Methods: Retrospective analysis of available data of patients who were rendered a histological diagnosis of genital porokeratosis. The database consisted of biopsies received in private consultation by the first author in the period January 2000 to March 2013. Results: Ten young men, 8 in their third decade, presented with pruritic plaques restricted to the peno-scrotal region of variable duration. The lesions were well-demarcated on the penis, but ill-defined with a rough granular surface on the scrotum. None of patients were diagnosed clinically as porokeratosis. The lesions were poorly responsive to topical steroid/antifungal treatment, but two patients showed partial improvement with oral isotretinoin. Biopsy in nine patients revealed multiple cornoid lamellae involving epidermis (6) and adnexal structures (3). One patient had a single cornoid lamella. Conclusion: The clinical and histological presentation of these patients is different from typical genital porokeratosis described in the literature and we postulate that these patients have an unusual porokeratotic reaction pattern of the epidermis with multiple cornoid lamellae.Introduction
Porokeratosis restricted to the genital region is rare with few cases described in the literature. Only two reports have appeared in Indian dermatological literature, [1],[2] which described four patients, one a female with porokeratosis on the vulva. [1] The largest series of 10 patients, all male, was described from Taiwan. [3]
The cases described have been considered to be plaque porokeratosis (Mibelli) with clinical presentation of annular plaques with central atrophy and a groove at the summit of a peripherally raised keratotic margin and histologically showing the presence of cornoid lamellae.
Histologically, the hallmark of porokeratosis is the presence of cornoid lamellae, which consist of columns of parakeratosis with the loss of the granular layer at the base of the column and pallor of the upper spinous keratinocytes with dyskeratotic cells. A few cornoid lamellae are seen in porokeratosis of Mibelli, usually one at either end of the sections. Multiple cornoid lamellae have been described arising from adnexal structures in lesions described as porokeratotic adnexal ostial nevus (PAON) which is a unifying term, which includes lesions that have involvement of eccrine and or follicular ostia. [4] Furthermore, the cornoid lamella is no longer considered to be specific for porokeratosis as it has been described in several unrelated conditions and is now considered as an epidermal reaction pattern. [5]
We describe 10 young males who presented with pruritic plaques on the peno-scrotal region of several months duration whose clinical appearance was not typical of porokeratosis of Mibelli. Biopsy showed multiple cornoid lamellae in nine patients, which in three cases were seen to arise from eccrine and follicular structures. Clinico-pathologically these cases do not correspond to typical plaque porokeratosis and we postulate that these cases represent an unusual, hitherto undescribed epidermal reaction pattern with multiple cornoid lamellae.
Methods
This is a retrospective analysis of available data of patients who were rendered a histological diagnosis of genital porokeratosis. The database consisted of biopsies received in private consultation by the first author in the period January 2000 to March 2013.
Results
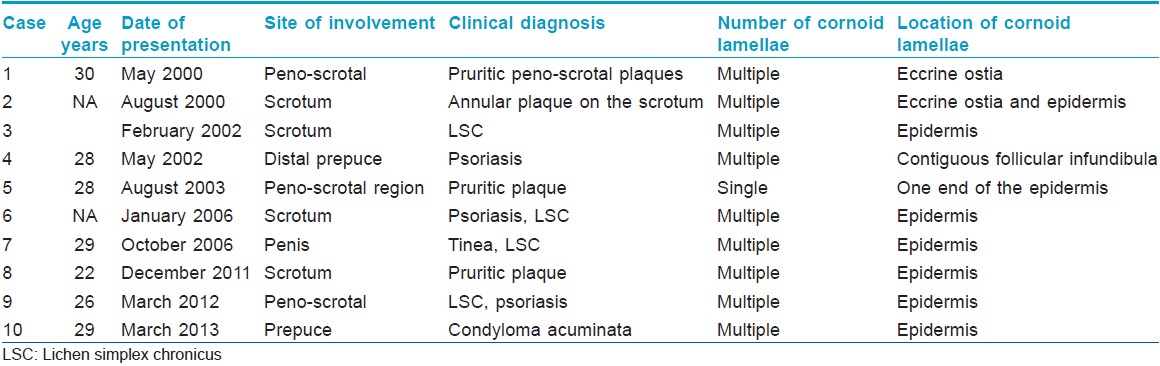
A total of 10 patients were identified, who had lesions restricted to the peno-scrotal region and who on biopsy showed features of porokeratosis, i.e., presence of cornoid lamellae. Detailed clinical descriptions were not available for all patients except Cases 1, 9 and 10. The results are tabulated in [Table - 1]. Most of the patients had the problem for several months before presentation and were lost to follow-up after variable periods of time.
Case 1 was a 30-year-old male patient who presented with a pruritic lesion on the ventral shaft of the penis sparing the mucosa. It was a fairly well defined, hourglass shaped plaque of about 5 cm by 2 cm in size, minimally elevated, with a rough granular surface marked by small spiny projections. The lesion was present since almost a year with a history of slow increase in its size. There was also involvement of the scrotum, which had a poorly demarcated involvement of the anterior part with a rough surface [Figure - 1]. Use of topical steroid preparations had given only temporary relief from the pruritus without any change in the size of the lesion.
 |
| Figure 1: Rough pebbly surface of scrotal skin and well demarcated plaque on distal prepuce. (healing biopsy site can be seen on scrotum) (Case 1) |
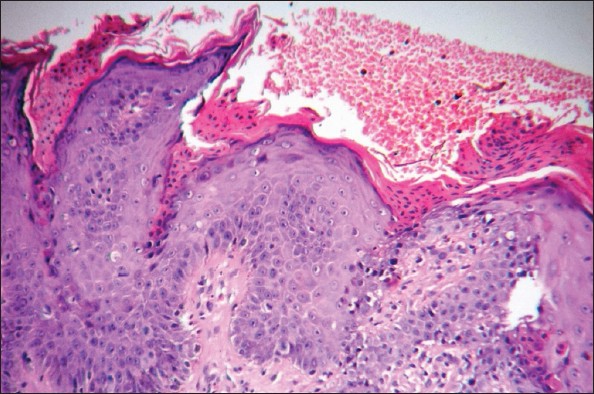
A biopsy from the lesion on the scrotum revealed multiple, equidistant, brightly eosinophilic columns of parakeratosis with keratotic spines that projected above the epidermal surface [Figure - 2]. These "cornoid lamellae" arose from epidermal invaginations that on serial sectioning were related to acrosyringia [Figure - 3]. The base of the parakeratotic columns had a markedly diminished or absent granular layer with slight vacuolization of surrounding cuticular cells and scattered dyskeratotic cells [Figure - 4].
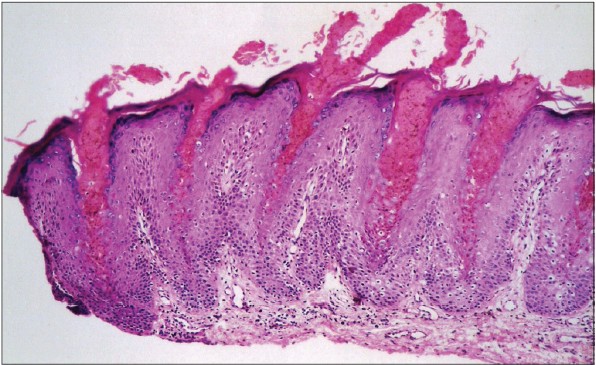 |
| Figure 2: Multiple bright pink columns of parakeratosis arising from contiguous eccrine acrosyringia with horny spines protruding above the surface of the epidermis (H and E, ×100) |
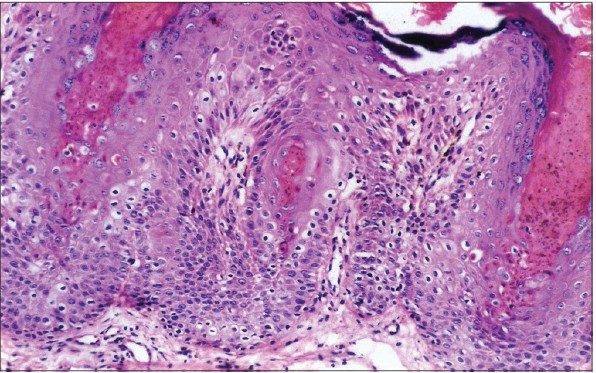 |
| Figure 3: Cornoid lamellae seen to involve an eccrine structure in the center of the sections (H and E, ×200) |
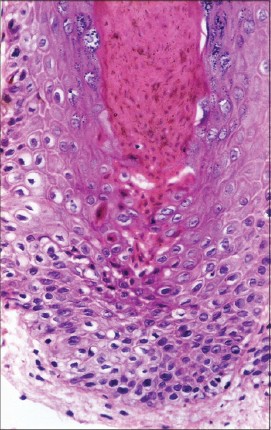 |
| Figure 4: Details of cornoid lamella with dyskeratotic cells at the base of the column of parakeratosis (H and E, ×400) |
Case 10, a 29-year-old man presented with a pruritic, fairly well-demarcated plaque, involving circumferentially the distal dorsal prepuce and extending onto the ventral surface without involvement of the glans. At places, there were tiny papular projections resembling condylomata acuminata, which was the clinical diagnosis [Figure - 5]. Biopsy findings showed multiple cornoid lamellae arising within a moderately hyperplastic epidermis.
 |
| Figure 5: Keratotic plaque over distal penis with papular excrescences (Case 10) |
A total of 4 patients had lesions restricted to the scrotum, three had lesions restricted to the distal penis while three cases had involvement of both the scrotum as well as the distal penis. Lesions on the penis were fairly well-circumscribed with easily discernible margins and a rough granular surface, however, no raised margin with a groove that is typical of porokeratosis was seen. The lesions on the scrotum mostly involved the anterior surface, were poorly circumscribed and had a diffuse rough granular surface. Clinically, most patients were labeled as pruritic plaques on scrotum and/or penis with lichen simplex chronicus, psoriasis and tinea as differential diagnoses. Patient 10 was thought to have condyloma acuminata due to the papillary projections on the surface of the lesion.
Nine patients had a similar histological picture with multiple cornoid lamellae that projected as horny spines above the surface of the lesion. The cornoid lamellae were seen to arise from eccrine structures in two cases and from follicles in one case. In case number two there was involvement of both eccrine acrosyringia as well as adjacent epidermis [Figure - 6]. Case number 5 had a single cornoid lamella located at one end of the sections, a finding that was at variance with the other nine cases and which was more akin to typical plaque type of porokeratosis.
 |
| Figure 6: Multiple cornoid lamellae involving epidermis and an acrosyringium at the right of the sections (H and E, ×100) (Case 2) |
Treatment with topical steroids and/or antifungals and oral antihistaminics was only partially helpful without any resolution of the condition. Cases 9 and 10 were put on oral isotretinoin and showed flattening of the lesions with a decrease in pruritus. The dose of isotretinoin used was 20 mg once daily and Case 9 had a recurrence of symptoms on discontinuation of the medication after 2 months, while Case 10 is still on treatment.
Dicussion
Genital porokeratosis is thought to represent plaque type of porokeratosis of Mibelli that is restricted to the genital region and clinically and histologically shares findings similar to plaque porokeratosis elsewhere on the body, namely, annular plaques with central atrophy and elevated thread like keratotic margins with a groove at the summit and which show one or a few cornoid lamellae on histopathology. Porokeratosis in general is not pruritic; however, pruritus was a presenting feature in most cases in the series of genital porokeratosis reported from Taiwan and was attributed to a hot and humid climate and repetitive trauma due to friction and scratching. [3] Genital porokeratosis has mainly been reported in males with very few case reports in females. [1],[6] The age of patients has varied from 27 to 75 years, unlike our patients eight out of 10 of whom were in their third decade with ages ranging from 22 to 30 years. The age of the remaining two patients was not recorded.
Most cases of genital porokeratosis reported in the literature were diagnosed as porokeratosis due to the typical clinical presentation. All our patients presented with itchy, fairly well-defined plaques on the penis and/or ill-defined lesions on the scrotum. None were diagnosed clinically as porokeratosis although the lesions on the penis did have well-defined margins. This may be because of lack of awareness as genital porokeratosis is a rare condition and pruritus is normally not a feature of porokeratosis.
Multiple cornoid lamellae have been described in porokeratotic eccrine ostial and dermal duct nevus and porokeratotic eccrine and hair follicle nevus where cornoid lamellae are seen to involve eccrine or follicular structures. Recently, the term PAON has been used to include both these entities. [4] Both conditions are thought to result from somatic mutations and may follow Blaschko′s lines. [4] Clinically, such patients present with acrally located keratotic papules, plaques or comedonal lesions.
Multiple cornoid lamellae have not been described in porokeratosis of Mibelli or in genital porokeratosis.
Cornoid lamellation while considered to be a fairly diagnostic finding in porokeratosis has also been reported in several unrelated conditions such as basal cell carcinoma, Bowens disease, seborrheic keratosis and verrucae and may be considered to be a reaction pattern of the epidermis [5] and not specific to porokeratosis.
A recent report [7] described a 48-year-old man with multiple pruritic erythematous scaly lesions on the face, which clinically did not resemble porokeratosis, but histologically had multiple cornoid lamellae and responded to topical steroid applications. The authors suggested that due to the discrepancies in morphology, distribution of lesions, symptomatology and response to therapy between their case and true porokeratosis, their case represented a new entity that is distinct from porokeratosis and the multiple cornoid lamellae possibly represent an unusual epidermal reaction pattern.
Nine of our cases had histological findings of multiple cornoid lamellae normally seen either in porokeratotic nevi or in a porokeratotic reaction pattern described earlier. [7] The age of our patients too, unlike previously reported cases is strictly restricted to the third decade. This age restriction to the third decade and combination of clinical features of pruritic plaques on the peno-scrotal region with multiple cornoid lamellae has not been reported earlier.
Although no common occupation or history of repeated exposure to hot humid environment was present in our patients it is possible that they have a common "porokeratotic" epidermal reaction pattern that has resulted in their lesions. Repeated minor frictional trauma due to tight fitting underclothes or a contact reaction to some agent may be factors in the pathogenesis of these lesions.
To conclude, we present 10 young males who presented with pruritic peno-scrotal plaques with multiple cornoid lamellae, a finding that has not been previously described.
We are not sure if our patients have genital porokeratosis with previously unreported histological finding of multiple cornoid lamellae or an unusual porokeratotic reaction pattern of the epidermis. We hope that awareness of this entity leads to more information on the nosology and pathogenesis of this condition.
| 1. |
Sengupta S, Das JK, Gangopadhyay A. Porokeratosis confined to the genital area: A report of three cases. Indian J Dermatol Venereol Leprol 2008;74:80.
[Google Scholar]
|
| 2. |
Dongre A, Adhe V, Sanghavi S. Genital porokeratosis: A rare entity. Indian J Dermatol 2013;58:81.
[Google Scholar]
|
| 3. |
Chen TJ, Chou YC, Chen CH, Kuo TT, Hong HS. Genital porokeratosis: A series of 10 patients and review of the literature. Br J Dermatol 2006;155:325-9.
[Google Scholar]
|
| 4. |
Goddard DS, Rogers M, Frieden IJ, Krol AL, White CR Jr, Jayaraman AG, et al. Widespread porokeratotic adnexal ostial nevus: Clinical features and proposal of a new name unifying porokeratotic eccrine ostial and dermal duct nevus and porokeratotic eccrine and hair follicle nevus. J Am Acad Dermatol 2009;61:1060.e1-14.
[Google Scholar]
|
| 5. |
Wade TR, Ackerman AB. Cornoid lamellation. A histologic reaction pattern. Am J Dermatopathol 1980;2:5-15.
[Google Scholar]
|
| 6. |
Robinson JB, Im DD, Jockle G, Rosenshein NB. Vulvar porokeratosis: Case report and review of the literature. Int J Gynecol Pathol 1999;18:169-73.
[Google Scholar]
|
| 7. |
Tran H, Bossenbroek NM, Rosenman K, Meehan SA, Sanchez M, Prystowsky S. Steroid-responsive facial eruption with cornoid lamellae - A possible new entity. Dermatol Online J 2008;14:9.
[Google Scholar]
|
Fulltext Views
4,018
PDF downloads
2,699





![[Table - 1]](#tbl_ijdvl_2014_80_1_24_125474_t7.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2014_80_1_24_125474_t1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_1_24_125474_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_1_24_125474_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2014_80_1_24_125474_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2014_80_1_24_125474_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2014_80_1_24_125474_f6.jpg){kind=link}