Translate this page into:
Janeway lesions - Revisited
2 Department of Pathology, Apollo Hospitals, Hyderabad, India
Correspondence Address:
Indukooru S Reddy
Department of Dermatology, Apollo Hospitals, Anand Sheel Enclave, Nandi Nagar, Banjara Hills, Hyderabad
India
| How to cite this article: Reddy IS, Gowrishankar S. Janeway lesions - Revisited. Indian J Dermatol Venereol Leprol 2013;79:136 |
Sir,
Osler′s nodes and Janeway lesions were described by William Osler in 1893 and Edward Janeway in 1899, in patients with bacterial endocarditis. During the pre-antibiotic era, extra cardiac physical findings such as Osler′s nodes and Janeway lesions were valuable clinical clues to the diagnosis of bacterial endocarditis. These lesions are now rarely observed because of early diagnosis and prompt treatment of infective endocarditis.
We report a 40-year-old male patient who was referred for dermatology consultation for asymptomatic skin lesions over the palms and soles since three days. Patient was hospitalised for high grade fever with chills, shortness of breath and productive cough. Dermatological examination showed multiple, discrete, erythematous, hemorrhagic macules, papules and few vesicles over palms, volar aspect of the fingers and soles [Figure - 1] and [Figure - 2]. Rest of the skin, mucus membranes and nails were within normal limits. Clinical examination of cardiovascular system did not reveal any abnormality. X-ray chest revealed consolidation of lower lobes of both lungs. Sputum, blood and skin lesions showed growth of methicillin-resistant staphylococcus aureus (MRSA). Conventional and transesophageal echocardiography did not show any evidence of endocarditis. Hematoxylin and eosin stained sections of skin biopsy obtained from palm showed epidermal necrosis, neutrophilic abscess in the reticular dermis and centre of the abscess showed clumps of gram positive coccobacilli [Figure - 3] and [Figure - 4]. The blood vessels did not reveal any evidence of vasculitis. Screening test for HIV was negative. Based on history, clinical examination and investigations, the diagnosis of Janeway lesions secondary to staphylococcal septicemia was made. Patient was treated with intravenous teicoplanin 200 mg twice daily for 3 days followed by 200 mg once a day for 10 days along with appropriate symptomatic measures. Patient recovered completely and skin lesions started resolving at the time of discharge.
 |
| Figure 1: Haemorrhagic macules and papules over the palms and volar aspect of the fingers |
 |
| Figure 2: Haemorrhagic macules over the medial aspect of the soles |
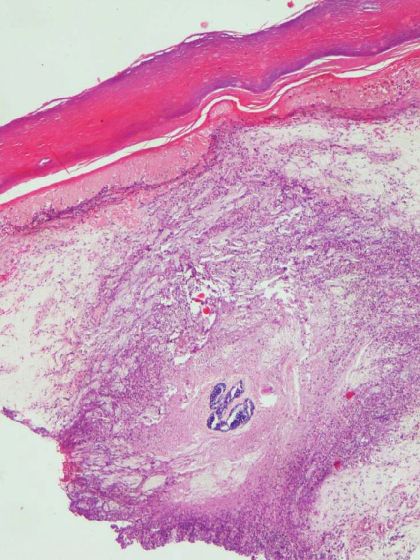 |
| Figure 3: Necrosed epidermis with a neutrophilic abscess in the reticular dermis with clumps of bacteria in the centre of the abscess (H and E, ×40) |
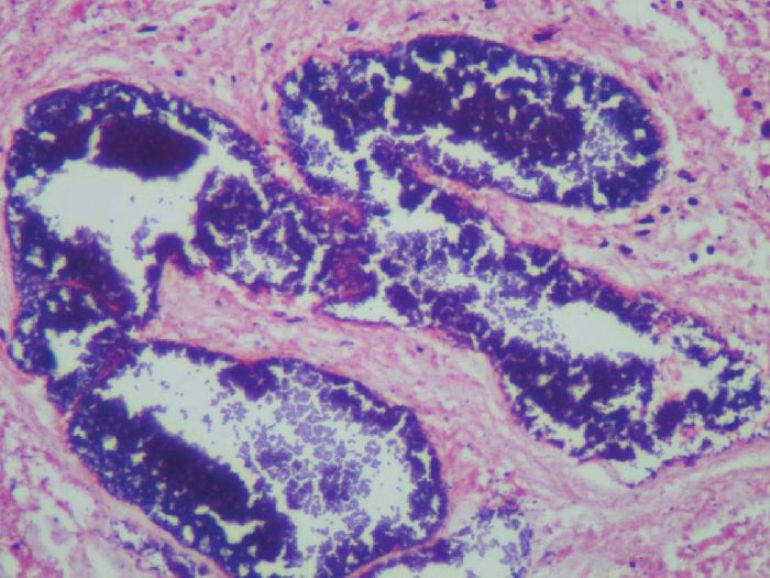 |
| Figure 4: High power view of the colonies of Staphylococci (H and E, ×400) |
The common cutaneous manifestations of bacterial endocarditis include Osler′s nodes, Janeway lesions, splinter haemorrhages and purpura. Osler′s nodes are painful, erythematous nodules with a pale centre, usually located on the pads of the fingers and toes. Janeway lesions are non tender, hemorrhagic macules, papules and nodules commonly seen over the palms and soles. [1] The exact pathogenesis of Osler′s nodes and Janeway lesions is not known. Initial reports documented perivascular infiltrate of neutrophils and endothelial swelling. [2] Hypersensitivity vasculitis to bacterial antigens was suspected. Subsequently, Alpert et al. suggested that Osler′s nodes and Janeway lesions were identical in pathogenesis and were the result of septic emboli. [3] Von Gemmengen and Winkelman hypothesised that pain in Osler′s nodes was due to involvement of glomus body with sterile emboli. [4] Both the conditions show neutrophilic abscess in the dermis and the surrounding arterioles may show microemboli. Parikh et al. reported clumps of gram positive coccobacilli within the lumen of a thrombosed blood vessel in Osler nodes and Janeway lesions in a patient with acute bacterial endocarditis. [5] Though initially described in patients with bacterial endocarditis, Osler′s nodes and Janeway lesions have been reported in conditions such as systemic lupus erythematosus, haemolytic anemia, gonococcemia and typhoid fever. [6] The other diagnostic possibilities to be considered in an acutely ill patient with rash and fever are drug reactions, bacteremia due to meningococci, gonococci, staphylococci and pseudomonas, infections due to echo and coxsackie viruses, rickettsial infections such as Rocky mountain spotted fever, endemic and epidemic typhi.
This case is presented for its rarity and to the best of our knowledge, occurrence of Janeway lesions as a manifestation of methicillin resistant staphylococcus aureus septicemia in the absence of underlying endocarditis has not been reported in the literature. Though very rare, these lesions still do occur and their recognition is important in the diagnosis of underlying sepsis.
| 1. |
CardulloAC, Silvers DN, Grossman ME. Janeway lesions and Osler's nodes: A review of histopathologic findings. J Am Acad Dermatol 1990;22:1088-90.
[Google Scholar]
|
| 2. |
Lian C, Nicolau S,Poincloux P.Histopathologie de nodule d Osler: e tude sur l' endotheliiite de l' endocardite maligne a evolution lente. Press Med 1929;37:497-9.
[Google Scholar]
|
| 3. |
Alpert JS, Krous HF, Dalen JE, O'Rourke RA, Bloor CM. Pathogenesis of Osler's nodes. Ann Intern Med 1976;85:471-3.
[Google Scholar]
|
| 4. |
Von Gemmengen GR, Winkelman RK. Osler's nodes of subacute bacterial endocarditis. Arch Dermatol 1967;95:91-4.
[Google Scholar]
|
| 5. |
Parikh SK, Liberman A, Colbert DA, Silvers DN, Grossman ME. The identification of methicillin-resistant Staphylococcus aureus in Osler's nodes and Janeway lesions of acute bacterial endocarditis. J Am Acad Dermatol 1996;35:767-8.
[Google Scholar]
|
| 6. |
Johnston GA, Graham-Brown RA. Skin manifestations of internal organ disorders. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller SA, Leffell D, editors. Fitzpatrick's Dermatology in general medicine. 7th ed, vol. 2. New York: McGraw Hill; 2008. p. 1445-60.
[Google Scholar]
|
Fulltext Views
7,394
PDF downloads
4,164





![[Figure - 1]](#fig_ijdvl_2013_79_1_136_104693_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_1_136_104693_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2013_79_1_136_104693_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2013_79_1_136_104693_f4.jpg){kind=link}