Translate this page into:
Minimal erythema dose to targeted phototherapy in vitiligo patients in Indian skin
Correspondence Address:
C Shanmuga Sekar
Department of Dermatology, PSG Hospitals, Coimbatore
India
| How to cite this article: Sekar C S, Srinivas CR. Minimal erythema dose to targeted phototherapy in vitiligo patients in Indian skin. Indian J Dermatol Venereol Leprol 2013;79:268 |
Sir,
Conventional phototherapy is useful in patients with extensive disease, but unnecessary exposure of uninvolved skin to radiation occurs in patients with limited disease. Targeted phototherapy is a hand-held device, which can deliver UV radiation over specific areas.
Minimal erythema dose (MED) is defined as the UV dose required to elicit just perceptible erythema 24 h after a single UV-exposure. [1] There are no strict guidelines regarding the determination of MED in vitiliginous skin before starting conventional phototherapy. As vitiliginous skin is akin to type 1 skin, it is natural to believe that the dosimetry should be uniform irrespective of the skin photo-type. Many patients with vitiligo have leathery skin over exposed areas induced by UVB. In few patients, the degree of depigmentation may vary, and they are likely to show different MED′s at different sites. Since targeted phototherapy involves delivering high doses for faster therapeutic effect, determination of MED becomes pivotal before starting therapy.
Thirty-two patients with localized vitiligo were selected for the study. The machine used was non-excimer UVB lamp emitting light in the range of 300 to 320 nm with a peak emission of 305 nm (Levia targeted phototherapy machine [Figure - 1]). The patients back was exposed to increasing radiation starting from 100 mj with increments of 50 mj over 6 sites during each sitting, and the MED was determined after 24 hours [Figure - 2]. We have used arithmetic series instead of geometric series, as it is easy to compute for MED determination. Treatment was started at 1 MED, and increments were made by 0.5 MED every sitting.
 |
| Figure 1: Levia targeted phototherapy system |
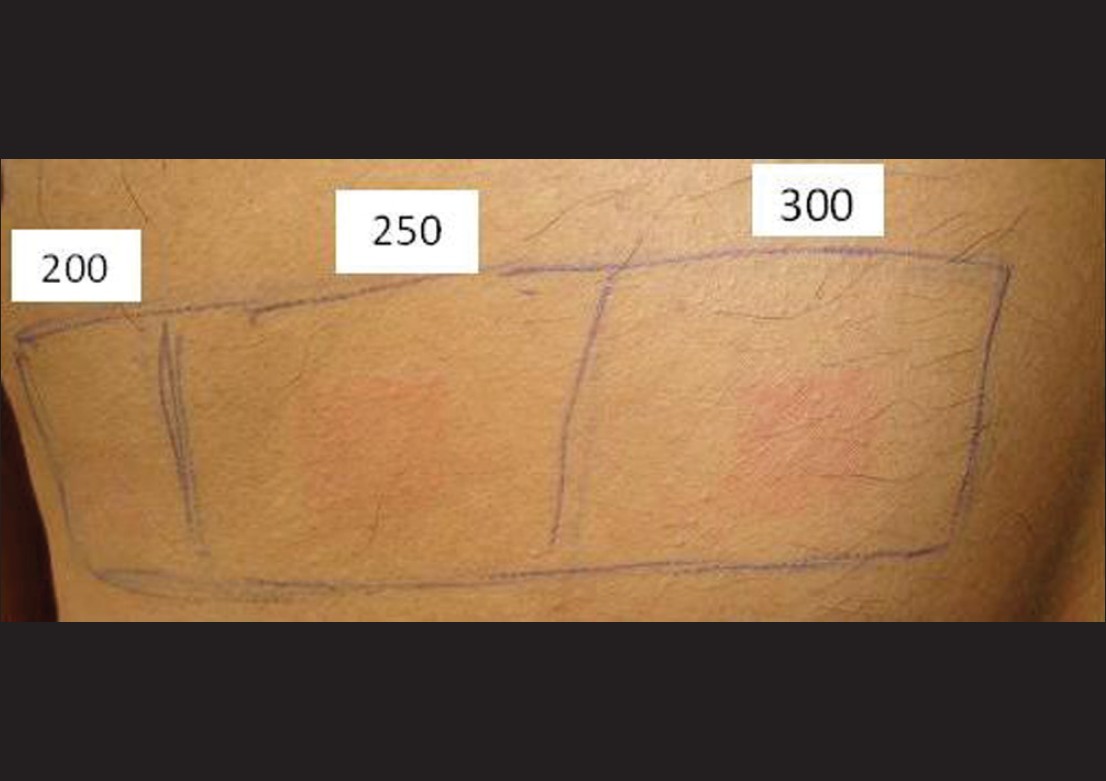 |
| Figure 2: MED determination (200 mj) |
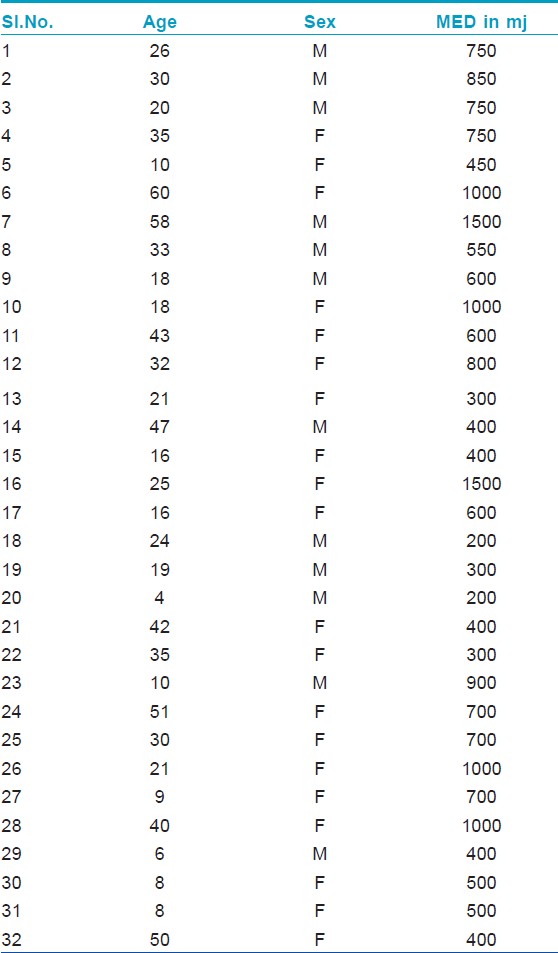
The results are tabulated in [Table - 1]. Out of 32 patients, there were 20 females and 12 males. The youngest patient was 4-year-old, and the oldest was 60-years-old. The patients belonged to type IV- VI Fitzpatrick skin type. The lowest MED recorded was 200 mj, and the highest was 1500 mj. The mean MED was 656 mj, and the median and mode were 600 mj and 400 mj, respectively.
Pai et al.[2] reported average MED for NBUVB for type IV to be 600 mj and type V skin to be 1100 mj. Tejaswi et al.[3] reported average MEDs to be 1000 mj/cm 2 for type IV and 750 mj/cm 2 for type V skin and concluded that the median MED for type V skin was lesser than that for type IV skin. Serish et al.[4] calculated the MED using broad band and narrow band UV light and found the mean MED to be 21 mj for BBUVB and 300 mj for NBUVB light.
The Fitzpatrick classification is not reliable in Indian skin since many patients with fair skin involved in outdoor occupation were reported to have high MED. [5] Similarly, women have low MED irrespective of skin pigmentation when compared to men of the same Fitzpatrick type (personal communication). Treating all patients as Fitzpatrick type 1 is acceptable when whole body is treated with NBUVB. However, when treating with targeted phototherapy, the idea is to deliver erythmogenic doses. In our experience, many patients have received up to 6 MEDs without blistering, and these patients will not respond if treated using low MED as starting point. The question arises as to how reliable MED determination over normal skin is useful in delivering treatment for vitiliginous skin. The practical difficulty of determining MED in vitiliginous skin is the degree of depigmentation may vary, and most patients needing targeted phototherapy do not have lesions large enough to permit MED determination over affected skin.
To conclude, MED determination is important before starting treatment with targeted phototherapy. This paper is not meant to provide guidelines for the treatment of vitiligo but to highlight that MED can vary, and hence treatment should be individualized
Coherent systems provided equipment for the study.
| 1. |
Ravnbak MH, Wulf HC. Pigmentation after single and multiple UV-exposures depending on UV-spectrum. Arch Dermatol Res 2007;299:25-32.
[Google Scholar]
|
| 2. |
Pai GS, Vinod V, Krishna V. Med estimation for narrow band UV-B on type IV and type V skin in India. Indian J Dermatol Venereol Leprol 2002;68:140-1.
[Google Scholar]
|
| 3. |
Tejasvi T, Sharma VK, Kaur J. Determination of minimal erythemal dose for narrow band-ultraviolet B radiation in north Indian patients: Comparison of visual and Dermaspectrometer® readings. Indian J Dermatol Venereol Leprol 2007;73:97-9.
[Google Scholar]
|
| 4. |
Serish, Srinivas CR. Minimal erythema dose (Med) to narrow band ultraviolet - B (NB-UVB) broad band ultraviolet-B (BB-UVB) - A pilot study. Indian J Dermatol Venereol Leprol 2002;68:63-4.
[Google Scholar]
|
| 5. |
Acharya S, Srinivas CR, Shenoi SD. Determination of minimal erythema does in Indian patient for ultraviolet B therapy. Indian J Dermatol Venereol Leprol 1991;57:214-5.
[Google Scholar]
|
Fulltext Views
5,323
PDF downloads
1,788





![[Figure - 1]](#fig_ijdvl_2013_79_2_268_107666_f2.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_2_268_107666_f3.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2013_79_2_268_107666_t1.jpg){kind=link}