Translate this page into:
A rare cause of oral papillomatous lesions: Cowden syndrome
2 Department of Internal Medicine, Faculty of Medicine, Mustafa Kemal University, Antakya-Hatay, Turkey
3 Department of Pathology, Faculty of Medicine, Mustafa Kemal University, Antakya-Hatay, Turkey
Correspondence Address:
Didem Didar Balci
Department of Dermatology, Faculty of Medicine, Mustafa Kemal University, 31100, Antakya-Hatay
Turkey
| How to cite this article: Balci DD, �elik M M, �elik E, Demir M, Yaldiz M. A rare cause of oral papillomatous lesions: Cowden syndrome. Indian J Dermatol Venereol Leprol 2012;78:230 |
Sir,
Cowden syndrome (multiple hamartoma syndrome) is a rare autosomal-dominant inherited disorder characterized by multiple hamartomatous neoplasms of ectodermal, mesodermal and endodermal origin with systemic involvement. [1],[2] Here, we present a 53-year-old female patient with the main complaint of multiple oral papillomatous lesions, which are the pathognomonic diagnostic criteria of Cowden syndrome.
A 53-year-old female patient presented with complaints of papules at the corners of the mouth, on the tongue and on the upper and lower gingiva. She reported that the papules in the mouth had appeared in her 20s, while those at the corners of the mouth had appeared 3 years ago. The lesions at the corners of the mouth had been cauterized a year earlier, but had recurred. There was no similar family history. Her dermatologic examination revealed multiple papules on the dorsal surface of the tongue, with a cobblestone appearance, as well as on the lower and upper gingiva and verrucous papules at the angles of the mouth [Figure - 1] and [Figure - 2]. Additionally, bilateral skin-colored papillomas in the postauricular region (one papilloma in each side) and bilateral nodular lesions on the dorsal surface of the feet (one nodule in each side) were observed.
 |
| Figure 1: Multiple papules on the dorsal surface of the tongue with a cobblestone appearance and verrucous papules at the bilateral anguli oris |
 |
| Figure 2: Papillomatous lesions on the upper gingiva and the mucosal surface of the upper lip |
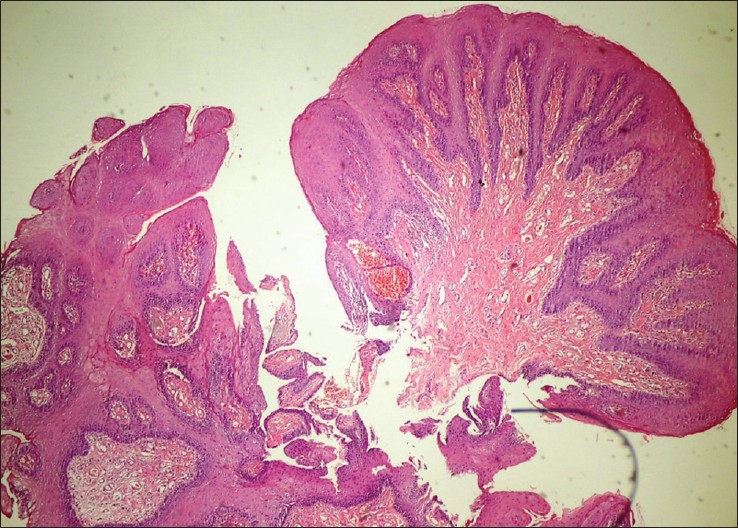 |
| Figure 3: Parakeratosis, acantosis and there is often some inward turning of the elongated rete ridges (H and E, ×40) |
Incisional biopsies obtained from the oral mucosa and anguli oris revealed parakeratosis and acantosis, and there is often some inward turning of the elongated rete ridges "squamous cell papillomatous lesion" [Figure - 3]. Excisional biopsy obtained from the retroauricular region revealed "fibroma molle." The lesions on the dorsal surface of the feet were considered as lipoma according to the histopathological findings of excisional biopsy. The fine-needle aspiration biopsy of the thyroid gland performed due to the observation of nodular formation on thyroid ultrasonography was reported as "benign cytology, cystic goiter." On endoscopic examination, multiple polyps, 2-3 mm in size, were observed in the stomach, and a biopsy revealed "hyperplastic polyp." The patient had minimal thoracic kyphosis as an additional systemic finding. Clinical examination, laboratory tests and imaging did not reveal intracranial pathology or any pathologic finding in the breast, eyes and genitourinary system.
Cowden syndrome was first described by Lloyd and Dennis in 1963, and they named this syndrome after the surname of their patient, Rachel Cowden. [3] Clinical diagnostic criteria were first proposed by Salem and Steck in 1983 and then revised and published by the International Cowden Consortium in 1995 and 2000. [2],[4]
According to the International Cowden Consortium (2000), facial trichilemmomas, acral keratoses, mucosal lesions and papillomatous papules constitute the pathognomonic criteria of the syndrome, whereas major criteria for the syndrome include breast cancer, thyroid cancer, endometrial cancer, macrocephaly and Lhermitte-Duclos disease. Minor criteria of the syndrome include thyroid lesions (goiter, follicular adenoma and thyroglossal duct cyst), mental retardation, gastrointestinal hamartomas (hyperplastic inflammatory, hamartomatous, adenomatous and lipomatous polyps), fibrocystic breast disease, lipoma, fibroma, genitourinary tumor and malformations. Skeletal system, nervous system, cardiopulmonary system and ophthalmologic findings may accompany in some cases. [1],[2] The diagnosis of Cowden syndrome is established in the following conditions: presence of pathognomonic lesions (if only mucocutaneous lesions are present as pathognomonic lesions: ≥6 facial papules, of which ≥3 must be trichilemmomas; cutaneous facial papules and papillomatosis in oral mucosa; papillomatosis in oral mucosa and acral keratosis; ≥6 palmoplantar keratosis lesions), presence of two major criteria, one of which must be macrocephaly, presence of one major criterion and three minor criteria and presence of four minor criteria [1],[5] Our case had multiple papillomas in the oral mucosa and bilateral verrucous papules at anguli oris, which are pathognomonic mucocutaneous findings. Among the minor criteria, benign cystic goiter and hamartomatous polyps in the gastrointestinal tract were determined in our case. Additionally, the present case had fibroma molle and lipoma as other skin findings of the syndrome. There was no intracranial, genitourinary or ophthalmologic pathology or any pathologic finding in the breast.
Multiple traumatic fibromas, oral fibromas in tuberous sclerosis, Darier-White disease, Heck′s disease, lymphangioma, pyogenic granuloma, fibroepithelial polyps, lipoid proteinosis, oral florid papillomatosis, oral papillomas in Goltz syndrome, mucosal neuromas of multiple endocrine adenomatosis, acanthosis nigricans, pseudoepitheliomatous hyperplasia and squamous cell carcinoma should be considered in the differential diagnosis of oral papillomatous lesions. [6]
Mammography at regular intervals and monthly breast self-examination are of importance for the early diagnosis of breast cancer. Some authors suggest bilateral prophylactic mastectomy. [7] Thyroid functions tests, thyroid ultrasonography, complete blood count, complete urine analysis, PAP smear test and abdominopelvic ultrasonography should be performed in all patients at the first step, and repeated at regular intervals. If thyroid nodules are present, fine-needle biopsy or surgical biopsy should be performed. [5] Our patient was also informed and put on a regular follow-up for colon polyps, thyroid nodules and breast diseases.
The responses of facial papules to different treatment modalities, including topical 5-fluorouracil, oral retinoids, curettage, electrosurgery, cryosurgery, laser ablation and surgical excision, are variable. [1],[8] Cryotherapy was performed for the papules at anguli oris, and fibroma molle in the retroauricular region were excised.
Patients with Cowden syndrome require lifelong follow-up, and family members should be screened for the disease. In conclusion, although cases of Cowden syndrome are rarely encountered, early diagnosis would decrease the associated mortality and morbidity.
| 1. |
Bayliss SJ, Dogramacý AC. Other Genodermatoses. In, Bolognia JL, Jorizzo JL, Rapini RP, editors. Dermatology, 2 nd ed. Spain: Mosby; 2008. p. 857-61.
[Google Scholar]
|
| 2. |
Eng C. Will the real Cowden syndrome please stand up: Revised diagnostic criteria. J Med Genet 2000;37:828-30.
[Google Scholar]
|
| 3. |
Lloyd KM 2 nd , Dennis M. Cowden's disease: A possible new symptom complex with multiple system involvement. Ann Intern Med 1963;58:136-42.
[Google Scholar]
|
| 4. |
Salem OS, Steck WD. Cowden's disease (multipl hamartoma and neoplasia syndrome): A case report and review of the English literature. J Am Acad Dermatol 1983;8:686-96.
[Google Scholar]
|
| 5. |
The NCCN 1. 2009 Cowden syndrome clinical practise guidelines in oncology. National Comprehensive Cancer Network. Available from: http://www.nccn.org. [cited in 2009].
[Google Scholar]
|
| 6. |
Fistarol SK, Anliker MD, Itin PH. Cowden disease or multipl hamartoma syndrome-cutaneous clue to internal malignancy. Eur J Dermatol 2002;12:411-21.
[Google Scholar]
|
| 7. |
Hartmann LC, Schaid DJ, Woods JE. Efficacy of bilateral prophylactic mastectomy in women with a family history of breast cancer. N Engl J Med 1999;340:77-84.
[Google Scholar]
|
| 8. |
Farooq A, Walker LJ, Bowling J, Audisio RA. Cowden syndrome. Cancer Treat Rev 2010;36:577-83.
[Google Scholar]
|
Fulltext Views
5,012
PDF downloads
4,222





![[Figure - 1]](#fig_ijdvl_2012_78_2_230_93666_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_2_230_93666_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_2_230_93666_f3.jpg){kind=link}