Translate this page into:
Achromatic atrophic macules and patches of upper extremities
2 Oracle Skin Clinic, Daegu, Korea
Correspondence Address:
Joon S Park
Department of Dermatology, College of Medicine, Catholic University of Daegu, 3056-6,Daemyung-4-Dong, Nam-gu, Daegu
Korea
| How to cite this article: Park JS, Chae IS, Kim IY, Ko DK, Chung H, Lee SW. Achromatic atrophic macules and patches of upper extremities. Indian J Dermatol Venereol Leprol 2013;79:270 |
A 55 year old man presented with numerous round achromatic atrophic macules and patches varying in diameter from 0.5-1 cm on his both arms [Figure - 1]. The lesions first appeared 4 months earlier and gradually increased in number. The lesions later became atrophic. There was no history of using drugs and topical corticosteroids. The rest of his general examination was unremarkable. A potassium hydroxide preparation showed numerous pseudomycelial hyphae and yeast cells with typical ′spaghetti and meatballs′ appearance [Figure - 2].
 |
| Figure 1: Numerous round achromatic atrophic macules and patches varying in diameter from 0.5-1 cm on the arm |
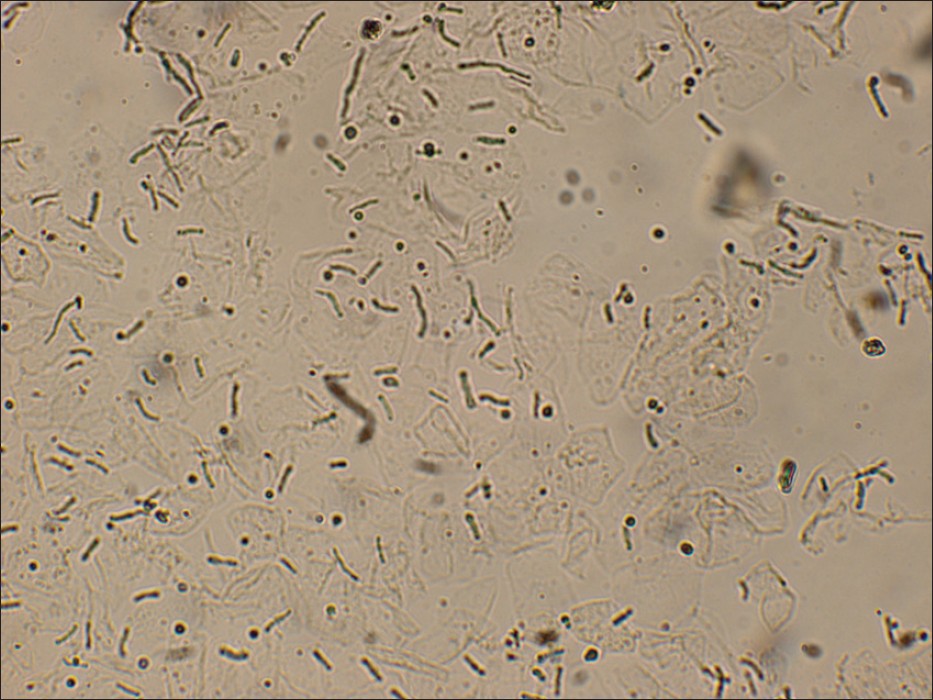 |
| Figure 2: Multiple short hyphae and spores shows 'Spaghetti and meatball' appearance in a KOH preparation |
Punch biopsies were done: One from the atrophic lesion [Figure - 3]a and the other from the normal skin. The biopsy specimen of the atrophic lesion revealed multiple short hyphae and spores in the cornified layer [Figure - 3]a whereas fungal elements were not observed from the normal tissue [Figure - 3]b. Retiform effacement, epidermal thinning, and mild periadnexal lymphocytic infiltration were present. Verhoeff′s elastic stain showed no alteration of elastic fibers in the dermis compared with that of normal tissue. The patient was treated with oral itraconazole (200 mg daily for 3 weeks) and showed improved atrophic lesions and mycological recovery.
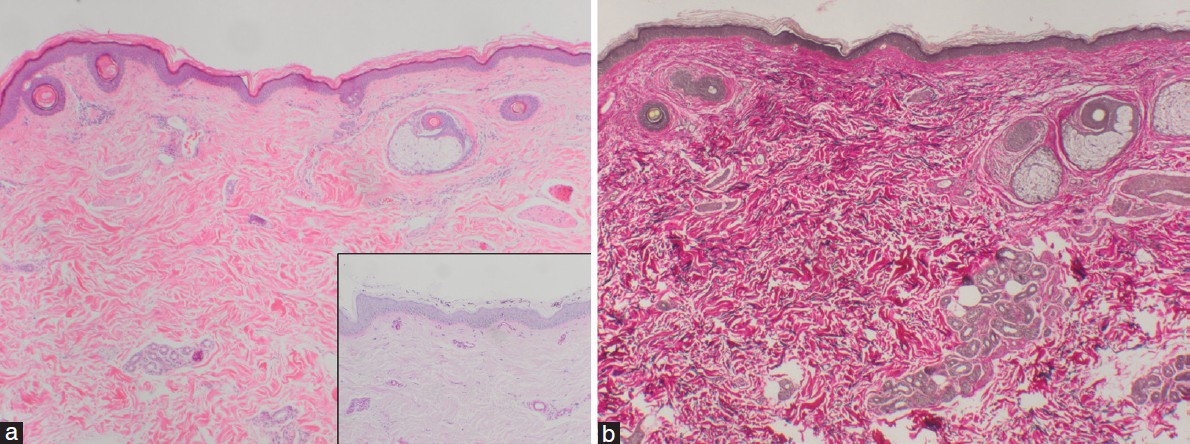 |
| Figure 3: (a) Histopathologic examination of atrophic lesion shows retiform effacement with epidermal thinning (H and E, × 40); inset with biopsy specimen of atrophic lesion shows multiple short hyphae and spores visible in the cornified layer (PAS stain, × 100); (b) Histopathologic examination of atrophic lesion shows no alteration of elastic fibers in the dermis (Verhoeff's elastic stain, × 40) |
What is your Diagnosis?

| 1. |
Faergemann J, Fredriksson T. Tinea versicolor: Some new aspects on etiology, pathogenesis, and treatment. Int J Dermatol 1982;21:8-11.
[Google Scholar]
|
| 2. |
Crowson AN, Magro CM. Atrophying tinea versicolor: A clinical and histological study of 12 patients. Int J Dermatol 2003;42:928-32.
[Google Scholar]
|
| 3. |
Romano C, Maritati E, Ghilardi A, Miracco C, Mancianti F. A case of pityriasis versicolor atrophicans. Mycoses 2005;48:439-41.
[Google Scholar]
|
| 4. |
Yang YS, Shin MK, Haw CR. Atrophying pityriasis versicolor: Is this a new variant of pityriasis versicolor? Ann Dermatol 2010;22:456-9.
[Google Scholar]
|
| 5. |
Tatnall FM, Rycroft RJ. Pityriasis versicolor with cutaneous atrophy induced by topical steroid application. Clin Exp Dermatol 1985;10:258-61.
[Google Scholar]
|
Fulltext Views
3,722
PDF downloads
1,867





![[Figure - 1]](#fig_ijdvl_2013_79_2_270_107677_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_2_270_107677_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2013_79_2_270_107677_f3.jpg){kind=link}