
Translate this page into:
Association between interleukin-17F rs763780 polymorphism and psoriasis risk: A meta-analysis
Corresponding author: Dr. Zhi Xiang, Jiangwangmiao Street, Nanjing, Jiangsu 210 042, China. xiangzhi0870@sina.com
-
Received: ,
Accepted: ,
How to cite this article: Xiang Z, Hao Z, Cui P, Lin L, Chen M, Chen PM. Association between interleukin-17F rs763780 polymorphism and psoriasis risk: A meta-analysis. Indian J Dermatol Venereol Leprol 2022;88:150-5.
Abstract
Background:
The polymorphism of interleukin-17F rs763780 has been found to have a probable association with increased risk of developing psoriasis.
Aims:
This study aims to get a more convincing estimation of the association between the interleukin-17F rs763780 T /C polymorphism and psoriasis risk.
Methods:
Two authors independently searched the databases including PubMed, EMBASE, Cochrane Central Register of Controlled Trials, Chinese National Knowledge Infrastructure, Wanfang and Chinese Biomedical Literature Databases for case–control studies which reported the odds ratios with 95% confidence intervals comparing genotype and allele frequencies of the interleukin-17F rs763780 polymorphism in patients with psoriasis versus participants without psoriasis.
Results:
A total of seven case–control studies incorporating 1824 cases and 1585 controls were identified. The pooled odds ratios indicated that interleukin-17F rs763780 C allele was a risk factor for psoriasis in allele frequency, recessive model and homozygote model (P < 0.05). Subgroup analysis by ethnicity further indicated that the C allele was closely related to increased risk of psoriasis in Asian populations (P < 0.05), but not in Caucasians.
Limitations:
Only a few studies on the interleukin-17F rs763780 polymorphism in psoriasis have been reported till date, thus the data is insufficient. Only one gene polymorphic site was selected for this study, and it is not clear whether other genetic mutation functional sites affect the gene. Further studies on confounding effects of other genetic polymorphisms are needed.
Conclusion:
The present meta-analysis results suggested that the interleukin-17F rs763780 T /C is significantly associated with psoriasis risk in Asians.
Keywords
Interleukin-17 rs763780
gene polymorphism
meta-analysis
psoriasis

Plain Language Summary
Interleukin (IL)17F rs763780 is a putative single nucleotide polymorphism locus in the IL-17 genes affecting the transcriptional regulation and gene expression of IL-17. Whether IL-17F rs763780 T/C is associated with psoriasis risk would be of interest to the readers. This study is the first meta-analysis to examine the association IL17F rs763780 polymorphism with psoriasis. The results suggested that the IL17F rs763780 T/C was significantly associated with psoriasis risk in Asians.
Introduction
Psoriasis is a chronic inflammatory autoimmune skin disease characterised by erythematous and scaly skin plaques, affecting 0.5‒11.4% of adults and 1.4% of children worldwide.1,2 However, several studies have shown that there are differences between Asia and other regions, and the incidence of psoriasis in Asians is relatively low (0.3–1.2% in China).3
Psoriasis is associated with various comorbidities, including cardiovascular disease, diabetes, depression and anxiety.4-6 Quality of life can be negatively affected, leading to severe social, emotional and physical burdens.
The pathogenesis of psoriasis is complex and is considered to be strongly influenced by genetic and environmental factors. Genetic factors also play an important role in the clinical type, age of onset, severity and treatment response of psoriasis.7,8 Evidence now indicates that both the interleukin 23/T helper cell 17 and T helper cell 1 pathways are crucial in the pathogenesis of psoriasis.8-10
IL-17A and IL-17F are encoded by genes located on chromosome 6p12,11 and they share 50% homology.12 IL-17F plays a role in tissue inflammation by inducing the release of pro-inflammatory and neutrophil-mobilising cytokines and shares pro-inflammatory effects on keratinocytes and neutrophils with IL-17A.13,14 Interleukin-17F rs763780 T /C is a putative single-nucleotide polymorphism locus in the IL-17 gene which affects the transcriptional regulation and gene expression of IL-17. Recent studies have found that the single-nucleotide polymorphism of interleukin-17F rs763780 T /C is associated with increased psoriasis risk,15-17 but the results are inconsistent and inconclusive. Therefore, we aimed to get a more comprehensive and reliable result by conducting a meta-analysis of previously published studies involving interleukin-17F rs763780 T /C gene polymorphism and psoriasis susceptibility.
Material and Methods
Publication search strategy and inclusion criteria
We conducted a systematic review, in accordance with the preferred reporting items for systematic reviews and meta-analyses guidelines, of case–control studies on the association of psoriasis with interleukin-17F rs763780 T /C gene polymorphism. We did not apply for registration. Published literature search was independently performed by two authors in the following electronic databases: PUBMED, EMBASE, Cochrane Central Register of Controlled Trials, Chinese National Knowledge Infrastructure, Wanfang and Chinese Biomedical Literature Databases. The searched terms were ‘psoriasis,’ ‘interleukin-17F’ or ‘IL-17F,’ ‘polymorphism’ or ‘mutation’ or ‘SNP’ or ‘single-nucleotide polymorphism’ or ‘genotype,’ without restrictions on language. The deadline for publication search was 31st July 2020. Eligible studies were retrieved and examined carefully. Firstly, duplicates were detected, while the others were filtered by titles and abstracts. Full texts were reviewed if the abstracts matched our interest. The references of all eligible studies were retrieved manually for other potentially relevant studies. Inclusion criteria were: (a) Case–control design; (b) the association of interleukin-17F rs763780 polymorphism and psoriasis risk should be evaluated and (c) detailed data could be obtained to calculate odds ratios genotype and 95% confidence intervals. Non case–control studies, review articles or case reports were excluded. Figure 1 shows the preferred reporting items for systematic reviews and meta-analyses guidelines flowchart.

- The preferred reporting items for systematic reviews and meta-analyses guidelines flowchart
Data extraction quality assessment
Related information in each eligible study was independently and manually extracted by two investigators. The extracted information included the first author’s name, publishing year, country, ethnicity, genotyping method and genotype numbers of cases and controls. Discrepancies, if occurring during the data extraction, were resolved by a consensus achieved by the third author. The preferred reporting items for systematic reviews and meta-analyses guidelines process was followed for literature search and data extraction. The Newcastle-Ottawa scale was used to assess the quality of included studies.
Statistical analysis
The crude pooled odds ratio with 95% confidence intervals was used to evaluate the association between the interleukin-17F rs763780 polymorphism and psoriasis risk. The pooled odds ratios were calculated using dominant model (CC+TC vs. TT), recessive model (CC vs. TC+TT), homozygous model (CC vs. TT), heterozygous model (TC vs. TT) and allele genetic model (C vs. T). χ2 test was used to evaluate the Hardy–Weinberg equilibrium of the control group polymorphism. P < 0.05 was considered to be statistically significant indicating deviation from Hardy–Weinberg equilibrium. The statistical heterogeneity among studies was evaluated by Cochrane’s Q-test and I2 measurement. P ≤ 0.10 and I2 ≥50% showed significant heterogeneity. A random effect model was used in the incidence of significant heterogeneity; if not, a fixed effect model using the Mantel–Haenszel method was adopted. Stratified analysis was completed by ethnicity to evaluate the difference in odds ratio between studies of Caucasians and those of Asians. Sensitivity analysis was conducted to evaluate the validity and reliability of the primary meta-analysis. Forest plots graph was produced to estimate the pooled association between the interleukin-17F rs763780 and psoriasis risk. Statistical analysis was performed using Stata 12.0 software (Stata Corp., College Station, TX, USA), and P < 0.05 was considered as statistically significant.
Results
Characteristics of eligible studies
A total of 180 studies were obtained from literature search, 19 duplicates were removed and 130 studies were excluded for irrelevant topic and/or abstract. The remaining 31 studies were reviewed, of which 24 did not meet the inclusion criteria, including three reviews, four duplicated articles, three non case–control studies, ten of which were not related to IL-17F gene while four only involved patients with psoriasis arthritis. Finally, seven studies met the criteria, incorporating 1824 cases and 1585 controls.11,13,15-19 Characteristics of eligible studies are shown in Table 1.
| Author | Year | Country | Ethnicity | Sample size (male/female) | Genotype (case/control) | Allele (case/control) | Hardy–Weinberg equilibrium | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case | Control | TT | TC | CC | T | C | P-value | ||||
| Shibata | 2009 | Japan | Asian | 153 95/58 |
103 63/40 |
120/84 | 29/17 | 4/2 | 269/185 | 37/21 | 0.317 |
| Batalla | 2015 | Spain | Caucasian | 580 313/267 |
567 312/255 |
521/504 | 59/63 | 0/0 | 1101/1071 | 59/63 | 0.161 |
| Prieto-Perez | 2015 | Spain | Caucasian | 194 114/80 |
197 98/99 |
175/184 | 19/13 | 0/0 | 369/381 | 19/13 | 0.632 |
| Bialecka | 2016 | Poland | Caucasian | 407 212/195 |
205 98/107 |
385/196 | 22/9 | 0/0 | 792/401 | 22/9 | 0.747 |
| Kim | 2017 | Korean | Asian | 208 129/79 |
266 154/112 |
154/207 | 41/48 | 10/4 | 349/462 | 61/56 | 0.530 |
| Kaur | 2018 | Indian | Asian | 166 109/57 |
150 106/44 |
65/49 | 83/65 | 19/36 | 213/163 | 121/137 | 0.120 |
| Choi | 2019 | Korean | Asian | 116 64/52 |
97 47/50 |
90/85 | 24/12 | 2/0 | 204/182 | 28/12 | 0.516 |
Results of meta-analysis
No significant deviation from the Hardy–Weinberg equilibrium was observed for the single-nucleotide polymorphisms in controls (P > 0.05). Since CC genotype was absent in three European countries, four studies from Asia were analysed for recessive model and homozygote model, seven studies were included for all models analysis. Significant heterogeneities were observed in allele frequency model, homozygote model and recessive model (I2>50%), so we used random effect model. No significant heterogeneities were found in dominant model and heterozygote model, thus the fixed effect model was applied.
The pooled meta results were as follows: C versus T in allele frequency model odds ratio = 1.03 (95% confidence interval = 0.87–1.23), TC versus TT in heterozygote model odds ratio = 1.14 (95% confidence interval = 0.91–1.37), CC versus TT in homozygote model odds ratio = 0.82 (95% confidence interval = 0.40–1.35), CC versus TC+TT in recessive model odds ratio = 0.75 (95% confidence interval = 0.47–1.21) as well as CC+TC versus TT in dominant model odds ratio = 1.10 (95% confidence interval = 0.90–1.35), indicating that they were not associated with overall risk of psoriasis.
Heterogeneity and sensitivity analysis
Since major heterogeneities were observed in allele frequency model, homozygote model and recessive model, individual studies included in the meta-analysis were omitted consecutively to find the source through sensitivity analysis. When an original Indian study by Kaur et al. was omitted, the heterogeneities of above model were absent, and the results changed, indicating that study influenced the overall odds ratios values.17 By excluding this study, no heterogeneities were found among these three models. Overall odds ratios were as follows: Allele frequency model (C vs. T): Odds ratio = 1.25 (95% confidence interval = 1.01–1.53), P = 0.038, recessive model (CC vs. TC+TT): Odds ratio = 2.58 (95% confidence interval = 1.06–6.25), P = 0.037, homozygote model (CC vs. TT): Odds ratio = 2.65 (95% confidence interval = 1.10–6.42), P = 0.030, dominant model (CC+TC vs. TT): Odds ratio = 1.20 (95% confidence interval = 0.96–1.50), P > 0.05 and heterozygote model (TC vs. TT): Odds ratio = 1.15 (95% confidence interval = 0.92–1.44), P > 0.05. We did not measure the publication bias because it was inapplicable once the number of included studies was less than ten.
Subgroup meta-analysis of interleukin-17F rs763780 T /C polymorphism and psoriasis by ethnicity
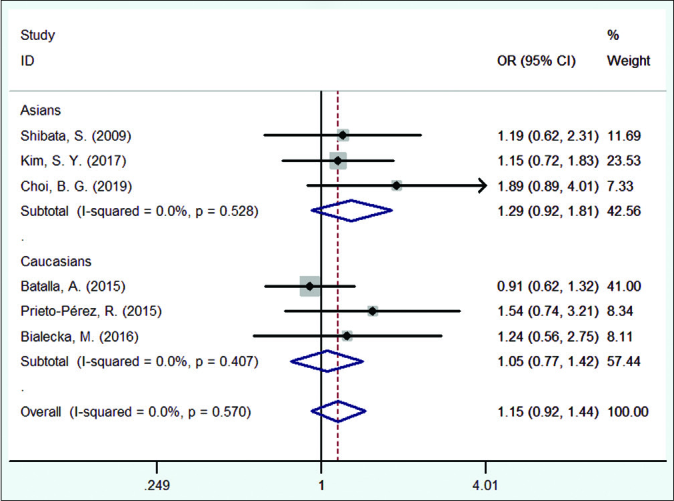
Subgroup analysis was conducted by ethnicity. In Asians subgroup, four studies were included. When the study by Kaur et al. was omitted, the heterogeneities were missing and the odds ratio results changed, indicating that the study affected the overall odds ratio values, so this study was excluded.17 Then, the meta-analysis results were as follows: Allele frequency model (C vs. T): Odds ratio = 1.47 (95% confidence interval = 1.10–1.97), P = 0.009, recessive model (CC vs. TC+TT): Odds ratio = 2.58 (95% confidence interval = 1.06–6.25), P = 0.037, homozygote model (CC vs. TT): Odds ratio = 2.65 (95% confidence interval = 1.10–6.42), P = 0.030, dominant model (CC+TC vs. TT): Odds ratio = 1.41 (95% confidence interval = 1.02–1.94), P = 0.038 and heterozygote model (TC vs. TT): Odds ratio = 1.29 (95% confidence interval = 0.92–1.81).
In Caucasians subgroup, three studies were included, meta-analysis results were as follows: Allele frequency model (C vs. T): odds ratio = 1.04 (95% confidence interval = 0.77–1.41), dominant model (CC+TC vs. TT): Odds ratio = 1.05 (95% confidence interval = 0.77–1.42), heterozygote model (TC vs. TT): Odds ratio = 1.05 (95% confidence interval = 0.77–1.42). Analyses based on the recessive model, homozygote model and CC genotype versus TT or TC genotype showed no statistical significance because there was no CC genotype in the control as well as the patients group. Forest plot of pooled odds ratios and subgroup meta-analysis results are shown in Figure 2a-e.
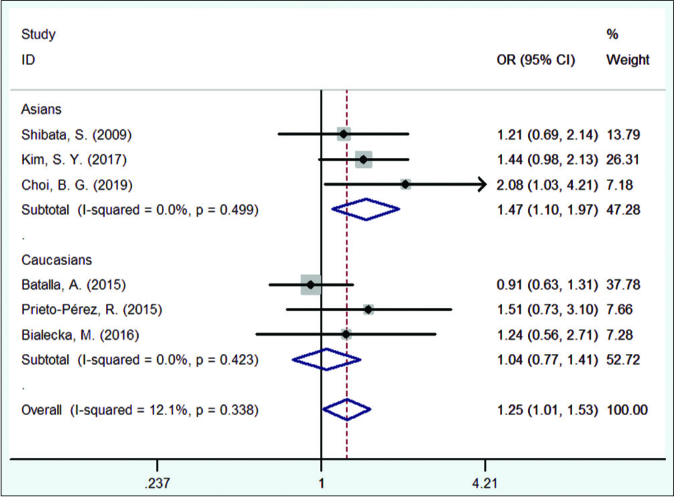
- Forest plot of the risk of psoriasis associated with IL17F gene rs763780 polymorphism in allele model
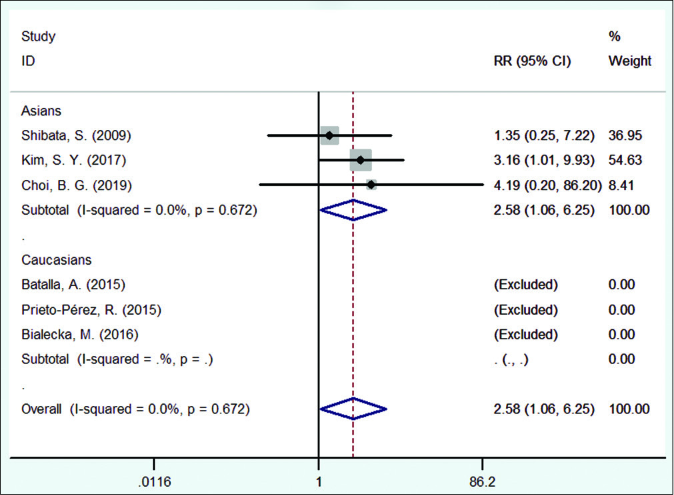
- Forest plot of the risk of psoriasis associated with IL17F gene rs763780 polymorphism in recessive model
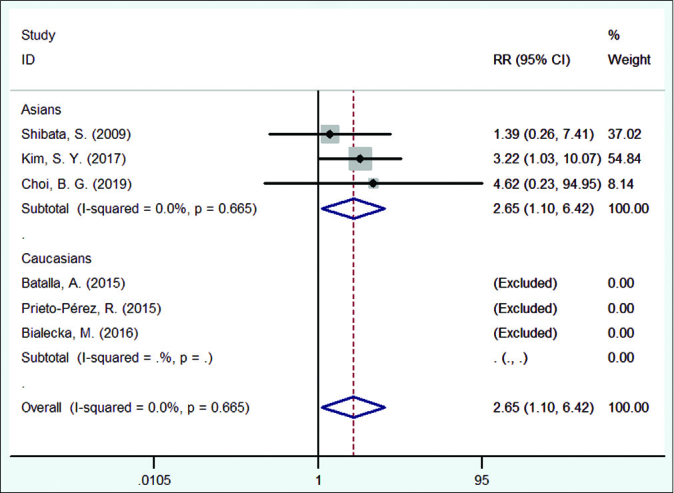
- Forest plot of the risk of psoriasis associated with IL17F gene rs763780 polymorphism in homozygous model
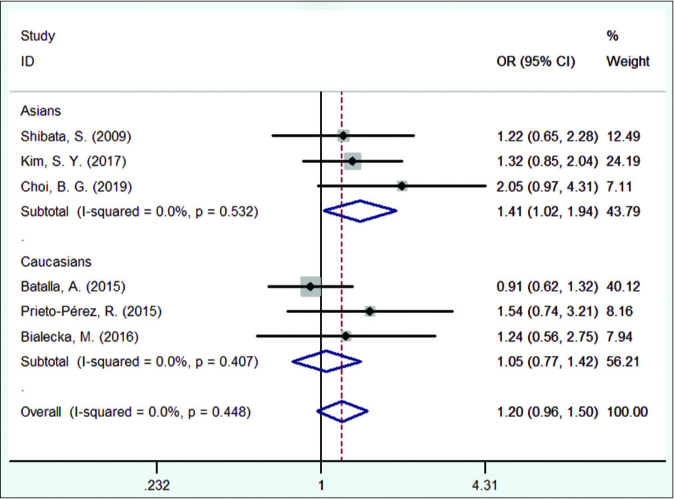
- Forest plot of the risk of psoriasis associated with IL17F gene rs763780 polymorphism in dominant model
- Forest plot of the risk of psoriasis associated with IL17F gene rs763780 polymorphism in heterozygote model
Discussion
The interleukin-17F gene, located on chromosome 6, encodes a protein related to the immune system which is specifically expressed in the mucosal and epithelial barrier to protect against some pathogens. Its main role is to recruit leukocytes, promote granulopoiesis and induce pro-inflammatory cytokines and chemokines in extracellular pathogens infections. It is expressed primarily in T lymphocytes and CD4+ monocytes after antigen activation.20,21
The single-nucleotide polymorphism of rs763780 in the interleukin-17F gene encoding IL-17F is a missense mutation, resulting in a histidine-to-arginine substitution at amino acid 161. According to Choi’s study, a significant increase in serum IL-12 levels was observed in psoriasis subjects harbouring the interleukin-17F polymorphism; thus they speculated that the increase in the IL-12 concentration was a secondary effect of increased IL-17F production.16 IL-17 and associated biomarkers activate immune cells, such as dendritic cells and macrophages, which produce IL-12.22,23 Sequence variations in specific nucleotides of interleukin-17F have a direct effect on the production of the encoded protein IL-17F. A newly published Egyptian study by Fouad et al. (at the time of our last search, we did not find this study, thus it was not included in the final analysis) had the similar findings which found that IL-17F serum level was significantly higher in psoriasis patients with mutant allele C compared to that with the wild T allele.24 Interleukin-17F polymorphism (rs763780) may influence the level of production of IL-17F with subsequent effects on the pathogenesis of psoriasis. Therefore, these two above studies suggested that the interleukin-17F rs763780 polymorphism was associated with increased risk of psoriasis by playing a critical role in the pathogenesis of psoriasis through its direct and indirect effects on the production of IL-17F and IL-12.16,24
We were unable to find any previous meta-analysis to examine the association between interleukin-17F rs763780 polymorphism and psoriasis. We found that interleukin-17F rs763780 polymorphism conferred an increased susceptibility to psoriasis in Asians, but not in Caucasians.
In Asians, the interleukin-17F rs763780 showed a more than two-fold increased prevalence in patients with psoriasis in recessive model (CC vs. TC+TT): Odds ratio = 2.58 and homozygote model (CC vs. TT): Odds ratio = 2.65, and one-fold increased prevalence in allele frequency model (C vs. T): Odds ratio = 1.47 and dominant model (CC+TC vs. TT): Odds ratio = 1.41. Our meta results suggested that homozygous carriers of the CC genotype had approximately a two-fold increase in the risk of psoriasis among Asians.
In our analysis, the CC genotypes were only detected in Asian countries. According to an Indian study, the highest CC genotype was found in 11.5% of psoriasis patients.17 Notably, the frequency of the CC genotype varied greatly among Asian controls (0% in Korea and 24% in India). No CC genotype was detected in European population. However, the TT genotype was more common in Caucasian patients (89–94%) than in Asians (39–78%), indicating that there was an ethnic difference in this single-nucleotide polymorphism.
Four Asian studies investigated the association between interleukin-17F rs763780 CC polymorphism and risk of psoriasis, one of which presented negative results. One possible explanation was that small sample size increased the possibility of false-positive or false-negative association caused by genotype of rs763780 polymorphism.
Interleukin-17F rs763780 T /C polymorphism has been studied in various diseases other than psoriasis. A meta-analysis conducted in 2017 reported that interleukin-17F rs763780 variant increased the rheumatoid arthritis risk.25 Genetic correlation between psoriasis and inflammatory bowel disease has also been identified. Patients with psoriasis had an increased risk of Crohn’s disease (risk ratio = 2.53) and ulcerative colitis (risk ratio = 1.71) from a meta-analysis conducted in 2018.26 According to a population-based nationwide study in Korea, patients with psoriasis consistently revealed higher standardised prevalence (age and sex adjusted) of inflammatory bowel disease compared to the general population. Severe psoriasis demonstrated higher odds of inflammatory bowel disease (odds ratio = 2.96) than mild psoriasis (odds ratio = 1.68).27
In addition, increased levels of IL-17 were found in both inflammatory bowel disease and psoriasis. This genetic polymorphism has been studied in patients with inflammatory bowel disease. In a study of a Chinese population with inflammatory bowel disease, the C variant was significantly more common in patients with Crohn’s disease, indicating an increased risk of Crohn’s disease development.28 However, a meta-analysis in 2017 concluded that the polymorphism was not associated with inflammatory bowel disease.25
In a functional study using recombinant wild-type and mutant IL-17F proteins, the C variant failed to induce pro-inflammatory cytokines and chemokines, nor could it antagonise the activity of wild-type IL-17F in bronchial epithelial cells, confirming that the C variant exerted a protective effect in asthma.29
Based on currently available data, it is clear that interleukin-17F rs763780 locus plays an important role in the human immune system, but the differences in risks or protective effects of various diseases in different populations require further investigation.
Recent clinical studies on psoriasis have implicated that IL-17 not only plays a significant role in psoriatic inflammation but also in treatment outcomes. In 2015, Prieto-Pérez et al. observed that interleukin-17F rs763780 TT genotype was associated with better response to ustekinumab and adalimumab during the six-month treatment period among psoriasis patients.11 On the contrary, carriers of the C allele were associated with better response to infliximab, suggesting that interleukin-17F rs763780 polymorphism was able to influence response to treatment.
Limitations
Very few studies on the interleukin-17F rs763780 polymorphism in psoriasis have been reported till now, not to mention small sample sizes, thus the data available is insufficient. Only three studies were included in our subgroup analysis, so results may be underpowered; further studies with larger samples are required. The variation in genetic background may have effects on the susceptibility to psoriasis; only one gene polymorphic site was selected for the study, but it is not clear whether other sites affect the gene. Future studies on the confounding effects of other genetic polymorphisms are recommended. More studies involving different nations and regions should be done. Finally, heterogeneity, publication bias and other confounding factors may confound our findings. We did not apply for registration and did not measure the risk of bias.
Conclusion
This study provides an inclusive meta-analysis of interleukin-17F rs763780 polymorphism with increased psoriasis risk. The results indicated that interleukin-17F rs763780 polymorphism was a risk factor for Asian psoriasis patients, but this association was not found in Caucasians. Therefore, further studies are needed to confirm these results in larger cohorts of multiethnic populations, to elucidate the true role of interleukin-17F rs763780 and other polymorphisms in psoriasis susceptibility.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A systematic review of worldwide epidemiology of psoriasis. J Eur Acad Dermatol Venereol. 2017;31:205-12.
- [CrossRef] [PubMed] [Google Scholar]
- A systematic review and meta-analysis of the efficacy and safety of the interleukin (IL)-12/23 and IL-17 inhibitors ustekinumab, secukinumab, ixekizumab, brodalumab, guselkumab and tildrakizumab for the treatment of moderate to severe plaque psoriasis. J Dermatolog Treat. 2018;29:569-78.
- [CrossRef] [PubMed] [Google Scholar]
- Comorbidities in psoriasis. Indian J Dermatol Venereol Leprol. 2013;79(Suppl 7):S10-7.
- [CrossRef] [PubMed] [Google Scholar]
- Psoriasis and comorbid diseases. J Am Acad Dermatol. 2017;76:377-90.
- [CrossRef] [PubMed] [Google Scholar]
- Gene polymorphisms that can predict response to anti-TNF therapy in patients with psoriasis and related autoimmune diseases. Pharmacogenomics J. 2013;13:297-305.
- [CrossRef] [PubMed] [Google Scholar]
- Pathophysiology of psoriasis. Indian J Dermatol Venereol Leprol. 2013;79(Suppl 7):S1-9.
- [CrossRef] [PubMed] [Google Scholar]
- The IL-23/Th17 Axis in the immunopathogenesis of psoriasis. J Invest Dermatol. 2009;129:1339-50.
- [CrossRef] [PubMed] [Google Scholar]
- Newer targeted therapies in psoriasis. Indian J Dermatol Venereol Leprol. 2013;79(Suppl 7):S47-52.
- [CrossRef] [PubMed] [Google Scholar]
- The polymorphism rs763780 in the IL-17F gene is associated with response to biological drugs in patients with psoriasis. Pharmacogenomics. 2015;16:1723-31.
- [CrossRef] [PubMed] [Google Scholar]
- The role of IL-17 in psoriasis. J Dermatolog Treat. 2015;26:41-4.
- [CrossRef] [PubMed] [Google Scholar]
- Association between single nucleotide polymorphisms IL17RA rs4819554 and IL17E rs79877597 and psoriasis in a Spanish cohort. J Dermatol Sci. 2015;80:111-5.
- [CrossRef] [PubMed] [Google Scholar]
- IL17RA gene variants and anti-TNF response among psoriasis patients. Pharmacogenomics J. 2018;18:76-80.
- [CrossRef] [PubMed] [Google Scholar]
- A preliminary study of new single polymorphisms in the T helper type 17 pathway for psoriasis in the Korean population. Clin Exp Immunol. 2017;187:251-8.
- [CrossRef] [PubMed] [Google Scholar]
- The IL17F His161Arg polymorphism, a potential risk locus for psoriasis, increases serum levels of interleukin-17F in an Asian population. Sci Rep. 2019;9:18921.
- [CrossRef] [PubMed] [Google Scholar]
- Association of genetic polymorphism of interleukin-17A and interleukin-17F with susceptibility of psoriasis. Indian J Med Res. 2018;148:422-6.
- [CrossRef] [PubMed] [Google Scholar]
- IL-17F single nucleotide polymorphism is not associated with psoriasis vulgaris or atopic dermatitis in the Japanese population. J Dermatol Sci. 2009;53:163-5.
- [CrossRef] [PubMed] [Google Scholar]
- IL17A and IL17F gene polymorphism association with psoriasis risk and response to treatment in a Polish population. Dermatology. 2017;232:592-6.
- [CrossRef] [PubMed] [Google Scholar]
- Cutting edge: IL-17F, a novel cytokine selectively expressed in activated T cells and monocytes, regulates angiogenesis and endothelial cell cytokine production. J Immunol. 2001;167:4137-40.
- [CrossRef] [PubMed] [Google Scholar]
- IL-17 cytokines in immunity and inflammation. Emerg Microbes Infect. 2013;2:e60.
- [CrossRef] [PubMed] [Google Scholar]
- Interleukin-12: Functional activities and implications for disease. Cytokine Growth Factor Rev. 2015;26:559-68.
- [CrossRef] [PubMed] [Google Scholar]
- The immunopathogenesis of psoriasis. Dermatol Clin. 2015;33:13-23.
- [CrossRef] [PubMed] [Google Scholar]
- Association of genetic variants of the interleukin-17F rs763780 and its circulating level in psoriasis patients in Egypt. Egypt J Immunol. 2020;27:39-46.
- [Google Scholar]
- Meta-analysis of risk association between interleukin-17A and F gene polymorphisms and inflammatory diseases. J Interferon Cytokine Res. 2017;37:165-74.
- [CrossRef] [PubMed] [Google Scholar]
- Association of psoriasis with inflammatory bowel disease. JAMA Dermatol. 2018;154:1417-23.
- [CrossRef] [PubMed] [Google Scholar]
- Psoriasis increases the risk of concurrent inflammatory bowel disease: A population-based nationwide study in Korea. Indian J Dermatol Venereol Leprol. 2019;845:145-52.
- [CrossRef] [PubMed] [Google Scholar]
- Genetic polymorphisms of interleukin 17A and interleukin 17F and their association with inflammatory bowel disease in a Chinese Han population. Inflamm Res. 2013;62:743-50.
- [CrossRef] [PubMed] [Google Scholar]
- IL-17F sequence variant (His161Arg) is associated with protection against asthma and antagonizes wild-type IL-17F activity. J Allergy Clin Immunol. 2006;117:795-801.
- [CrossRef] [PubMed] [Google Scholar]




