Translate this page into:
Asymptomatic cerebriform papules and nodules over left buttock
Correspondence Address:
Uday Khopkar
Department of Dermatology, Seth GS Medical College and KEM Hospital, Parel, Mumbai-400 012
India
| How to cite this article: Rameshwar G, Chikhalkar S, Mahajan S, Kharkar V, Khopkar U. Asymptomatic cerebriform papules and nodules over left buttock. Indian J Dermatol Venereol Leprol 2011;77:254 |
A 12-year-old female presented with a history of multiple asymptomatic raised lesions on the left buttock gradually increasing in size since one year. Cutaneous examination revealed multiple skin colored to slightly yellowish firm cerebriform sessile nodules and plaques over the left buttock extending up to the intergluteal cleft but not crossing the midline or not extending over lower back or upper thigh [Figure - 1] The lesions were nontender. Systemic examination revealed no abnormalities. Routine hematological and biochemical investigations were within normal limits. Histopathology showed a normal epidermis and islands of fat cells embedded among the collagen bundles in the reticular dermis and few of them extending as high as the papillary dermis. The collagen appeared to be normal with mild lymphocytic infiltrate in the dermis [Figure - 2].
 |
| Figure 1: Multiple skin colored cerebriform papules and nodules over left buttock |
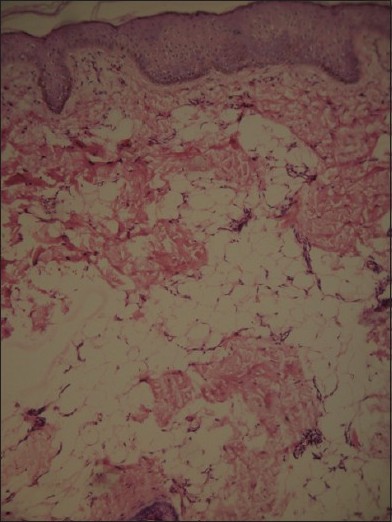 |
| Figure 2: Multiple mature adipocytes in the papillary and reticular dermis (H and E, ×200) |
What is your Diagnosis?
Diagnosis: Nevus lipomatosus cutaneous superficialis (NLCS) of Hoffman and Zurhelle
Histopathology showed a normal epidermis with multiple islands of adipocytes within the collagen bundles of the reticular dermis, replacing nearly 50% of the dermis. A few of these islands were located perivascularly in the papillary dermis. Some of the fat cells appeared immature but most of them were mature adipocytes. The collagen in the dermis appeared normal. A mild lymphocytic infiltrate was seen in the reticular dermis.
Discussion
As the name suggests, NLCS is a nevoid anomaly or hamartoma. It is a rare benign developmental anomaly characterized by the presence of mature adipose tissue in the dermis. It was first described by Hoffman and Zurhelle in 1921. [1] Clinically, it can be divided into two forms. The first or classical form, as described by Hoffman and Zurhelle, consists of multiple soft to cerebriform papules or nodules occurring in a segmental or zonal distribution. The second form occurs as a solitary papule or nodule. [2] The classical form has a predilection for the pelvic girdle with onset usually at birth or in childhood, whereas the solitary form is seen more commonly in adults and has no predilection for a particular anatomic area. The reason for the increased appearance of these growths in pelvic girdle is not known. [2],[3]
The exact pathogenesis of NLCS remains unknown. Various hypotheses have been discussed, including the possibility that these lesions arise from pre-adipose tissue or undifferentiated mesenchymal cells surrounding dermal blood vessels. Another theory is that a defect in dermal connective tissue leads to the deposition of fat cells in dermis. [2] Electron microscopy of four cases revealed a vascular origin of the abnormal adipose tissue found in the dermis. The young fat cells differentiated into mature fat cells in a process comparable to fetal adipogenesis. [4]
The lesions usually grow slowly as in our case but may reach a large size if not treated. The largest solitary NLCS reported was 20 Χ 30 cm. [5] A skin biopsy must be performed to confirm the diagnosis. The clinical differential diagnosis includes segmental neurofibromatosis in the case of zonal NLCS or a giant acrochordon with fatty herniation in the case of a solitary nodule. [2]
In Goltz syndrome(focal dermal hypoplasia) also, there is adipose tissue in the dermis but it can be differentiated by the absence of collagen and clinical appearance, associated abnormalities. Sometimes, dermal melanocytic nevi also show the presence of adipocytes in the dermis but additional presence of nests of nevus cells will help to differentiate it from NLCS. [5]
No systemic abnormalities, malignant change, familial or sex predilection have been noted with NLCS. [5] But connective tissue nevi, hemangiomas, angiokeratoma of Fordyce and some pigmentary disorders like cafe-au-lait macules, leukodermic spots, hypertrichosis and comedo-like lesions have been reported. [2],[5] No any such association was seen in our case.
Treatment is mainly for cosmetic purpose and surgical excision with primary closure is curative. Small lesions should be excised early in life to prevent excessive scarring in future. Our patient underwent surgical excision and most of the lesions healed with primary intention except the largest one that formed ulcer.
| 1. |
Umashankar T, Prasad T, Rajeshwari SH. Naevus lipomatosus superficialis: Clinicopathologic study of a case. Indian J Pathol Microbiol 2003;46:444-5.
[Google Scholar]
|
| 2. |
Al-Mutairi N, Joshi A, Nour-Eldin O. Naevus lipomatosus cutaneous superficialis of Hoffmann-Zurhelle with angiokeratoma of fordyce. Acta Dermatol Venereol 2006;86:92-3.
[Google Scholar]
|
| 3. |
Dhar S, Kumar B, Kaur I. Naevus lipomatosus superficialis of Hoffman and Zurhelle. Indian J Dermatol Venereol Leprol 1994;60:39-40.
[Google Scholar]
|
| 4. |
Raymond JL, Stoebner P, Amblard P. Nevus lipomatosus cutaneous superficialis: An electron microscopic study of four cases. J Cutan Pathol 1980;7:295-301.
[Google Scholar]
|
| 5. |
Chougule A, Kumari R, Thappa DM. Giant nevus lipomatosus cutaneous superficialis of the thigh. Indian J Dermatol 2007;52:120-1.
[Google Scholar]
|
Fulltext Views
3,197
PDF downloads
3,985





![[Figure - 1]](#fig_ijdvl_2011_77_2_254_77497_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_2_254_77497_f2.jpg){kind=link}