Translate this page into:
Blaschko-linear angioma serpiginosum
Correspondence Address:
Dipti Das
Flat No. 706, E Wing, Trans Residency 1, Subhash Nagar, MIDC, Road-23, Andheri East, Mumbai - 400 093, Maharashtra
India
| How to cite this article: Das D, Nayak CS, Tambe SA. Blaschko-linear angioma serpiginosum. Indian J Dermatol Venereol Leprol 2016;82:335-337 |
Sir,
Angioma serpiginosum is a rare, benign, nevoid vascular anomaly characterized by multiple, minute, bright red, grouped angiomatous spots arranged in linear arrays, small rings or serpiginous patterns.
A 19-year-old woman presented with asymptomatic reddish eruptions on the right upper limb for 6 years. The eruption started on the right arm and gradually progressed downward in a linear fashion to involve the right forearm as well. There was no history of trauma, contact allergy or bleeding from any site. Past history and family history were non-contributory.
Examination revealed multiple minute brightly erythematous grouped macules and irregular patches arranged in a serpiginous pattern extending from the right arm to right mid-forearm in a Blaschkoid distribution [Figure - 1]a and [Figure - 1]b, [Figure - 2]a,[Figure - 2]b,[Figure - 2]c,[Figure - 2]d. Lesions were non-blanchable on diascopy [Figure - 3]a. Mucocutaneous and systemic examination was unremarkable. Ophthalmological examination did not reveal any abnormality.
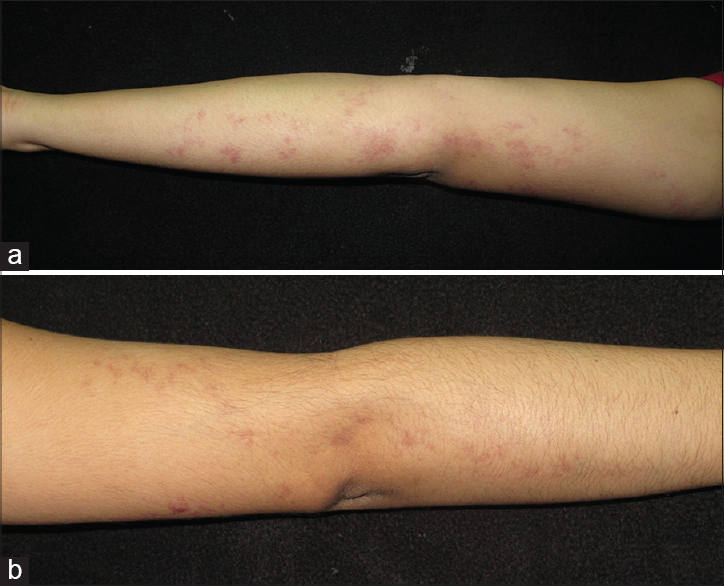 |
| Figure 1: (a and b) Multiple grouped, punctate, erythematous macules in a linear distribution following Blaschko's lines extending from right arm to right mid-forearm |
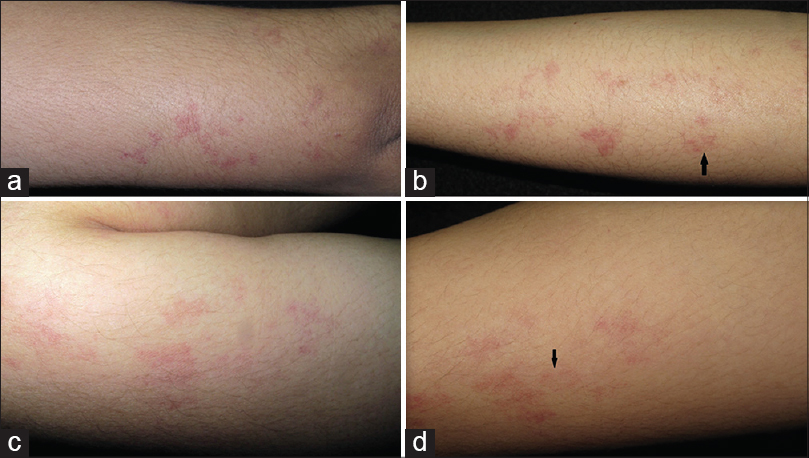 |
| Figure 2: (a-d) Close-up view of the lesion on right upper extremity showing grouped, punctate, erythematous macules and irregular patches, some are annular (arrow) |
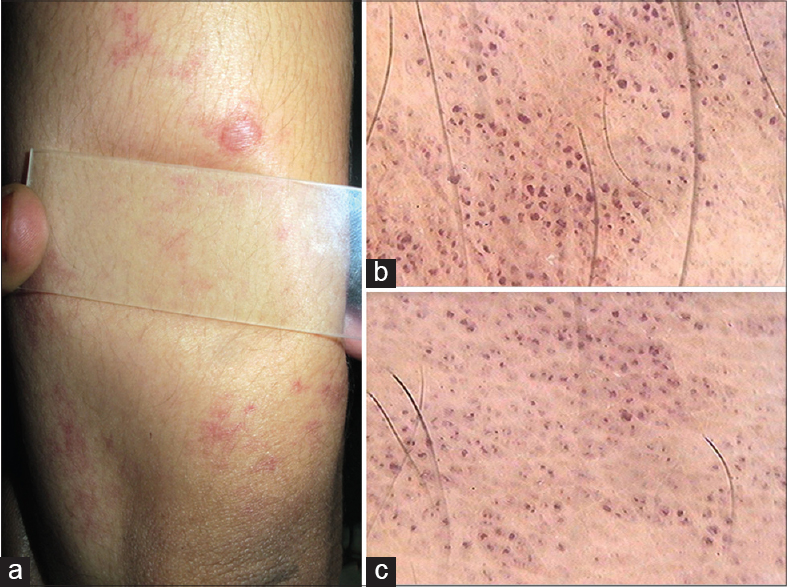 |
| Figure 3: (a) Non-blanchable lesions on diascopy. (b and c) Dermoscopy showing multiple well-demarcated red lagoons |
Laboratory investigations including complete hemogram and serum biochemistry profiles were within normal limits. On dermoscopy, multiple well-demarcated red lagoons were found [Figure - 3]b and [Figure - 3]c. Skin biopsy from the erythematous macules showed dilated capillaries in the dermal papillae and upper dermis. No inflammatory infiltrate or extravasation of red cells was observed [Figure - 4]a and [Figure - 4]b.
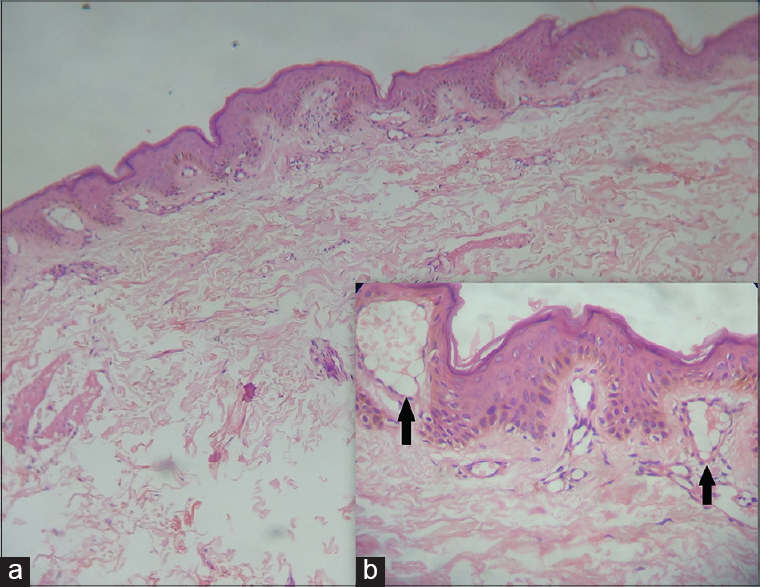 |
| Figure 4: (a) There are dilated capillaries in dermal papillae and upper dermis (H and E, ×100). (b) Dilated capillaries at higher power (H and E, ×400) |
Based on the clinical features, diascopy, dermoscopy and histopathological findings, a diagnosis of angioma serpiginosum was made. The patient was counseled regarding the benign nature of the condition and was advised pulse-dye laser therapy as she was cosmetically concerned.
Angioma serpiginosum was first described by Hutchinson in 1889 and was named by Crocker in 1894.[1] Clinically, lesions of angioma serpiginosum are characterized by multiple, minute copper-colored to bright red angiomatous puncta occurring in small clusters and sheets. The arrangement and extension of the lesions may produce a serpiginous pattern.
Although it affects both sexes at all ages, 90% occur in girls under the age of 16. Predominant sites of involvement are the lower extremities and buttocks though atypical sites such as breast and soles may also be involved. Extensive involvement has also been reported.[2],[3],[4] It is usually sporadic but familial occurrence has also been reported. Though the condition is limited mainly to skin, the ocular and nervous systems may also be involved.[5]
The pathogenesis of angioma serpiginosum is unknown. Increased levels of estrogen are postulated to play a role in the development of angioma serpiginosum because most cases arise in girls under 16 years of age and progress rapidly during pregnancy.[6]
Incomplete blanching occurs with pressure, but lesions are not purpuric.[7] The puncta represent dilated non-inflamed capillaries in the dermal papillae. These can be seen with dermoscopy.[7] Dermoscopy shows numerous small, relatively well-demarcated, round to oval red lagoons.[8]
Histopathology reveals dilated, thin-walled capillaries in some of the dermal papillae and the upper dermis. Epidermal changes and extravasation of red blood cells do not occur.
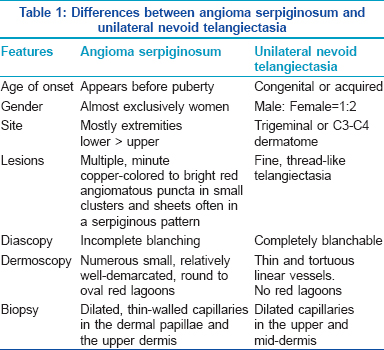
Differential diagnoses considered in our case were unilateral nevoid telangiectasia, pigmented purpuric dermatoses and port-wine stain. Unilateral nevoid telangiectasia presents as fine, thread-like telangiectatic lesions in a dermatomal distribution, usually involving unilateral C3 and C4 dermatomes and is completely blanchable [Table - 1]. Pigmented purpuric eruptions, particularly Majocchi's variant (purpura annularis telangiectoides) are more likely to be bilateral and show lymphocytes and extravasated erythrocytes on histopathologial examination. Port-wine stain is generally found unilaterally on the face and neck and is mostly localized in the distribution of the trigeminal nerve.
Angioma serpiginosum is slowly progressive and chronic. Spontaneous involution may occur but is never complete. Treatment with a pulsed dye laser may improve or eliminate such lesions. Early diagnosis of angioma serpiginosum may avoid unnecessary hematological work-up as the condition simulates purpura.
Linear or Blaschko-linear angioma serpiginosum appears to be a rare condition and we were able to find only a few previously published reports.[9],[10],[11],[12]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Hutchinson J. A peculiar form of serpiginous and infective naevoid disease. Arch Surg 1889;1:275.
[Google Scholar]
|
| 2. |
Mukherjee S, Salphale P, Singh V. Late onset angioma serpiginosum of the breast with co-existing cherry angioma. Indian Dermatol Online J 2014;5:316-9.
[Google Scholar]
|
| 3. |
Chen JH, Wang KH, Hu CH, Chiu JS. Atypical angioma serpiginosum. Yonsei Med J 2008;49:509-13.
[Google Scholar]
|
| 4. |
Katta R, Wagner A. Angioma serpiginosum with extensive cutaneous involvement. J Am Acad Dermatol 2000;42 (2 Pt 2):384-5.
[Google Scholar]
|
| 5. |
Gautier-Smith PC, Sanders MD, Sanderson KV. Ocular and nervous system involvement in angioma serpiginosum. Br J Ophthalmol 1971;55:433-43.
[Google Scholar]
|
| 6. |
Cox NH, Paterson WD. Angioma serpiginosum: A simulator of purpura. Postgrad Med J 1991;67:1065-6.
[Google Scholar]
|
| 7. |
Baker C, Kelly R. Other vascular disorders. In: Bolognia JL, Jorizzo JL, Schaffer JV, editors. Dermatology. 3rd ed. Philadelphia: Saunders Elsevier; 2009. p. 1754.
[Google Scholar]
|
| 8. |
Ilknur T, Fetil E, Akarsu S, Altiner DD, Ulukus C, Günes AT. Angioma serpiginosum: Dermoscopy for diagnosis, pulsed dye laser for treatment. J Dermatol 2006;33:252-5.
[Google Scholar]
|
| 9. |
Al Hawsawi K, Al Aboud K, Al Aboud D, Al Githami A. Linear angioma serpiginosum. Pediatr Dermatol 2003;20:167-8.
[Google Scholar]
|
| 10. |
Kalisiak MS, Haber RM. Angioma serpiginosum with linear distribution: Case report and review of the literature. J Cutan Med Surg 2008;12:180-3.
[Google Scholar]
|
| 11. |
Poenitz N, Koenen W, Utikal J, Goerdt S. Angioma serpiginosum following the lines of Blaschko – an effective treatment with the IPL technology. J Dtsch Dermatol Ges 2006;4:650-3.
[Google Scholar]
|
| 12. |
Chen W, Liu TJ, Yang YC, Happle R. Angioma serpiginosum arranged in a systematized segmental pattern suggesting mosaicism. Dermatology 2006;213:236-8.
[Google Scholar]
|
Fulltext Views
6,023
PDF downloads
2,330





![[Figure - 1]](#fig_ijdvl_2016_82_3_335_175916_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_3_335_175916_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_3_335_175916_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2016_82_3_335_175916_f4.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2016_82_3_335_175916_t5.jpg){kind=link}