Translate this page into:
Intralesional immunotherapy with tuberculin purified protein derivative for verruca: A study from a teaching hospital in South India
2 Department of Dermatology, Indira Gandhi Medical College and Research Institute, Puducherry, India
Correspondence Address:
Amit Shivaji Kerure
B-1, Mahagajanan CHS, Plot No. 19, Sec-9A, Vashi, Navi Mumbai - 400 703, Maharashtra
India
| How to cite this article: Kerure AS, Nath AK, Oudeacoumar P. Intralesional immunotherapy with tuberculin purified protein derivative for verruca: A study from a teaching hospital in South India. Indian J Dermatol Venereol Leprol 2016;82:420-422 |
Sir,
Cutaneous wart is a common skin disease and although multiple treatment options are available, none is completely effective.[1],[2] Recurrences after destructive treatment are common and can be frustrating. Immunotherapy with diphenylcyclopropenone and squaric acid dibutyl ester can cause allergic reactions. Risk of oncogenic potential of the virus is associated with autologous vaccine therapy.[3] Good therapeutic results were reported with immunotherapy using Candida, Trychophyton measles, mumps, rubella and tuberculin purified protein derivative antigens which are safe and inexpensive.[4]
We undertook a study over a period of 2½ years in the Department of Dermatology, Aarupadai Veedu Medical College and Hospital in Puducherry with the objective of studying the efficacy of tuberculin purified protein derivative antigens in clearance of warts. Patients with common warts as well as palmoplantar, periungual or facial warts were recruited. Subjects were enrolled in the study based on the following inclusion criteria: (1) warts present at any site except oral and genital mucosa and (2) tuberculin skin test sensitivity (induration ≥5 mm at 48 h). Exclusion criteria were (1) oral and genital mucosal warts, (2) patients below 12 years and above 65 years of age or (3) induration measuring <5 mm at 48 h of tuberculin skin test, which implied inadequate sensitivity to purified protein derivative antigen or anergy and hence the patient was unlikely to mount an adequate immune response necessary for clearance of warts.
Tuberculin purified protein derivative was injected intralesionally by an insulin syringe at a dose of 10 IU (0.1 mL) in the largest wart or the lesion most accessible at the first visit. It was then injected into the same lesion every 2 weeks until all lesions disappeared or for a maximum of six treatments. The size of warts at the injected site and that of other lesions were noted and distant warts were observed at follow-up visits. Patients were followed up for at least 3 months after the last treatment to look for recurrence of warts or the development of new warts.
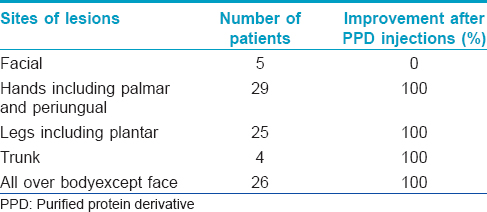
Out of a total of 110 patients with single or multiple warts that were included, 21 patients did not comply with the protocol and were thus excluded from the study. Their age ranged from 12 years to 52 years (mean age 24 years). The number of warts were one to more than 20. Sixty five out of the 89 patients included in the study had more than one lesion located at different sites. Eighty-four (94.4%) patients showed complete resolution with this immunotherapy protocol [Figure - 1],[Figure - 2],[Figure - 3]. Five patients with only facial warts showed no response even after six injections. [Table - 1]. Six patients (7%) showed a complete resolution of warts with a single injection. The median number of injections was 4. In all patients with multiple warts, the injected lesion as well as distant lesions that were not treated also disappeared. The only side effect reported was immediate pain due to injection. During the follow-up period, no patient developed new warts at the same site or any another site.
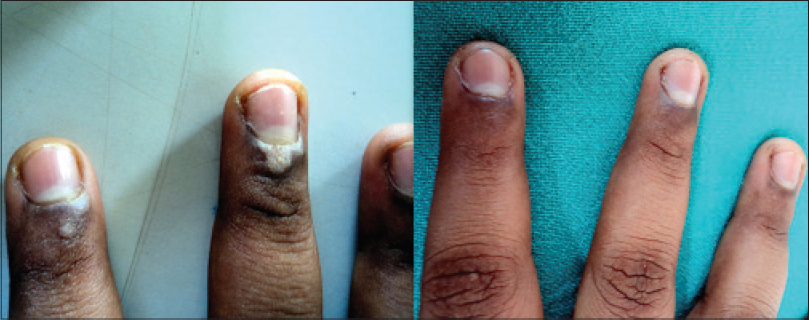 |
| Figure 1: Periungual warts before and after three injections of tuberculin purified protein derivative |
 |
| Figure 2: Verruca before and after four injections of tuberculin purified protein derivative |
 |
| Figure 3: Verruca before and after four injections of tuberculin purified protein derivative |
Intralesional immunotherapy is associated with production of Th1 cytokines which activate cytotoxic natural killer cells.[5],[6] Injection of antigen to which the patient was previously sensitized stimulates the elicitation phase of the immune response by enhancing the ability of the immune system to recognize human papilloma virus antigens. The immunostimulation is generalized which helps in clearing distant warts as well.
Abd-Elazeim et al. in a recent study, reported that there was a statistically significant increase in interleukin-12 of patients treated with purified protein derivative versus a control group[7] and complete clearance was seen in 75% of the cases. Nofal et al. reported complete clearance of the lesions in 63% patients and partial response in 23% patients with measles, mumps, rubella antigen.[6] Johnson and Horn found that intralesional immunotherapy using mumps or Candida antigens is an effective treatment for cutaneous warts.[8] Wananukul et al. and Kus et al. in separate studies used tuberculin purified protein derivative as antigens and reported a success rate of 50–93%.[1],[4] No severe adverse reactions were reported in these studies.
In our study, 84 (94.4%) patients showed clearance of lesions. The response rate in this study was much higher than in previous studies done elsewhere. Widespread prevalence of tuberculosis in our country and a mandatory Bacillus Calmette–Guérin (BCG) vaccination in the Indian population may be the reasons for the higher rate of clearance of warts in our patients (Indian population appears to be more sensitive to purified protein derivative compared to western populations). We found that the accumulated cure rate increased with increasing number of injections and was 100% after six injections. The limitations of our study are that no control group was included and warts in children below 12 years were not studied.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Wananukul S, Chatproedprai S, Kittiratsacha P. Intralesional immunotherapy using tuberculin PPD in the treatment of palmoplantar and periungual warts. Asian Biomed 2009;3:739-43.
[Google Scholar]
|
| 2. |
Lipke MM. An armamentarium of wart treatments. Clin Med Res 2006;4:273-93.
[Google Scholar]
|
| 3. |
Chandrashekar L. Intralesional immunotherapy for the management of warts. Indian J Dermatol Venereol Leprol 2011;77:261-3.
[Google Scholar]
|
| 4. |
Kus S, Ergun T, Gun D, Akin O. Intralesional tuberculin for treatment of refractory warts. J Eur Acad Dermatol Venereol 2005;19:515-6.
[Google Scholar]
|
| 5. |
Ibrahum MA, Ahmed RE, Al Sadar M. Intradermal vs intralesional purified protein derivatives in treatment of warts. Gulf J Dermatol 2011;18:21-25.
[Google Scholar]
|
| 6. |
Nofal A, Salah E, Nofal E, Yosef A. Intralesional antigen immunotherapy for the treatment of warts: Current concepts and future prospects. Am J Clin Dermatol 2013;14:253-60.
[Google Scholar]
|
| 7. |
Abd-Elazeim FM, Mohammed GF, Fathy A, Mohamed RW. Evaluation of IL-12 serum level in patients with recalcitrant multiple common warts, treated by intralesional tuberculin antigen. J Dermatolog Treat 2014;25:264-7.
[Google Scholar]
|
| 8. |
Johnson SM, Horn TD. Intralesional immunotherapy for warts using a combination of skin test antigens: A safe and effective therapy. J Drugs Dermatol 2004;3:263-5.
[Google Scholar]
|
Fulltext Views
4,234
PDF downloads
2,189





![[Figure - 1]](#fig_ijdvl_2016_82_4_420_175910_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_4_420_175910_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_4_420_175910_f3.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2016_82_4_420_175910_t4.jpg){kind=link}