Translate this page into:
Leser-Trelat sign with primary hepatic carcinoma
Correspondence Address:
Jiu-Hong Li
Department of Dermatology, No. 1 Hospital of China Medical University, 155 North Nanjing Street, Shenyang 110001, P. R.
China
| How to cite this article: Li JH, Guo H, Li B, Gao XH. Leser-Trelat sign with primary hepatic carcinoma. Indian J Dermatol Venereol Leprol 2015;81:320-321 |
Sir,
A 62-year-old male presented with a 3-year history of a brown patch on his face. Around the same time, several asymptomatic 1-2 cm sized brown spots began to appear on his checks. These were diagnosed as "age spots" at a local hospital and left untreated. One year ago, the number and the size of the lesions increased significantly and they gradually extended to the entire face, neck, chest, back and limbs. Though the lesions themselves continued to remain asymptomatic, he experienced right upper abdominal discomfort, fatigue, and weight loss (4 kg). His past medical history and family history were unremarkable.
General examination was unremarkable. Skin examination revealed numerous gray and brown, round to oval shaped, well-demarcated flat patches of variable sizes with a smooth surface, predominantly on the face, neck, and trunk, with a few similar lesions scattered on the limbs [Figure - 1]a-c. Some lesions were covered by light to dark brown crusts.
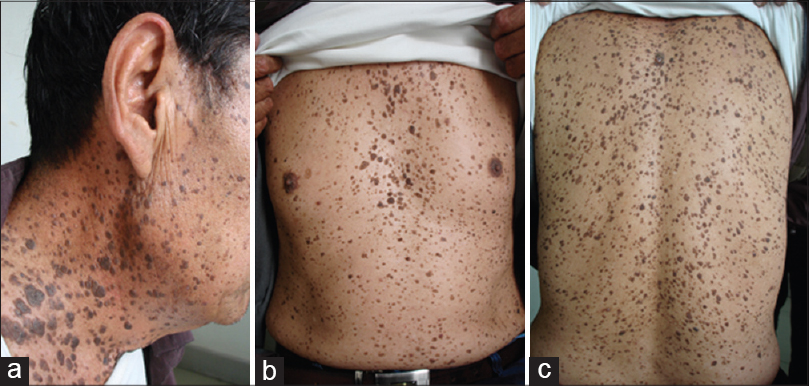 |
| Figure 1: Multiple eruptive seborrheic keratoses on the (a) face and neck, (b) breast, and (c) back |
A skin biopsy taken from one of the lesions on the back showed hyperkeratosis, acanthosis, and papillomatosis, consistent with seborrheic keratosis [Figure - 2]a. Investigations revealed the following: red blood cell count 3.4 × 10 9 /l, hemoglobin 85 g/l , platelet count: 11.3 × 10 9 /l, alanine transaminase 125 U/l, aspartate transaminase 541 U/l, alpha-feto protein 50 ng/dl, and negative HBsAg and anti-Hbe. Abdominal ultrasound demostrated several intrahepatic space occupying lesions. Magnetic resonance imaging (MRI) demonstrated an uneven hepatic surface, with a 5.9 × 5.7 cm, oval, well-defined hypointense mass in the right lobe; contrast-enhanced MRI showed an obvious non-homogeneous enhancement of the tumor in the arterial phase, washout of tumor in the portal venous phase and delayed phase, a low signal intensity of the mass compared to the increased signal intensity of the surrounding hepatic parenchyma, and multiple similar rounded nodules in the left and right lobes.
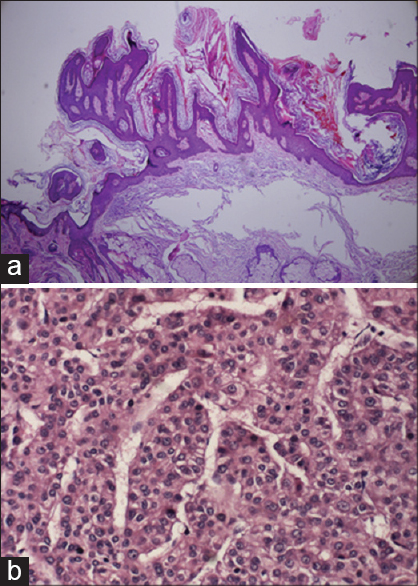 |
| Figure 2: (a) Skin biopsy taken from the lesion on the back showed pronounced hyperkeratosis and papillomatosis together with slight acanthosis (H and E x40). (b) Hepatic histopathological examination showed a large number of cells with nuclear atypia and enlarged nuclei (H and E x200) |
A biopsy of one of the hepatic tumour nodules demonstrated well differentiated hepatocytes containing bile pigment in the cytoplasm. The hepatocellular plates/cords were more than 2-3 cells thick, with a large number of cells showing nuclear atypia and enlarged nuclei [Figure - 2]b. The pathologic diagnosis was primary hepatic carcinoma.
The patient was treated by surgery. At 6-month follow-up, the lesions of seborrheic keratoses stopped progressing, but did not regress.
Leser-Trelat sign is defined as the association of the acute onset and/or rapid increase in the size and number of multiple seborrheic keratoses, with an underlying internal malignancy. Skin lesions of the Leser-Trelat sign are most often observed on the back and chest, followed by the extremities, face, and abdomen. [1] Common cancer entities associated with the Leser-Trelat sign include gastrointestinal adenocarcinomas, lymphoproliferative disorders, [2],[3] neoplasias of the breast, lung, urinary tract, [4] and ovarian cancer. [5] Leser-Trelat sign associated with hepatic carcinoma appears to be quite rare. Harrington [6] reported a 72-year-old man with Leser-Trelat sign associated with malignant hepatoma. Tajima [7] reported another case of a 57-year-old man who developed hepatocellular carcinoma and found the patient′s seborrhoeic keratoses erupted with the relapse of hepatocellular carcinoma, 1 year after intiial surgery.
Curth′s criteria developed by Helen Curth are particularly helpful to assess the relationship between unusual dermatoses and underlying malignancy. [8] According to the criteria, (1) the dermatosis is relatively uncommon; (2) it occurs with a specific neoplasm; (3) the two conditions are frequently observed together; (4) the onset is concurrent; (5) the condition takes a parallel course; and (6) the condition is not recognized as a part of a genetic syndrome. [8],[9],[10] Leser-Trelat sign is a relatively rare clinical condition found to be associated with internal malignancies. The skin lesions in our patient increased rapidly with the development of the underlying hepatic carcinoma and stopped increasing after the operation and thus satisfied some of Curth′s criteria.
Even though Leser-Trelat sign is rare, we recommend a comprehensive internal examination including that of the liver when patients present with multiple, rapidly evolving seborrhoeic keratoses.
| 1. |
Schwartz RA. Sign of Leser-Trelat. J Am Acad Dermatol 1996;35:88-95.
[Google Scholar]
|
| 2. |
Kurzrock R, Cohen PR. Cutaneous paraneoplastic syndromes in solid tumors. Am J Med 1995;99:662-71.
[Google Scholar]
|
| 3. |
Kilickap S, Yalcin B. Images in clinical medicine. The sign of Leser-Trelat. N Engl J Med 2007;356:2184.
[Google Scholar]
|
| 4. |
Heaphy MR Jr, Millns JL, Schroeter AL. The sign of Leser-Trelat in a case of adenocarcinoma of the lung. J Am Acad Dermatol 2000;43:386-90.
[Google Scholar]
|
| 5. |
Kebria MM, Belinson J, Kim R, Mekhail TM. Malignant acanthosis nigricans, tripe palms and the sign of Leser-Trelat, a hint to the diagnosis of early stage ovarian cancer: A case report and review of the literature. Gynecol Oncol 2006;101:353-5.
[Google Scholar]
|
| 6. |
Harrington CI. Leser-Trélat sign with porphyria cutanea tarda and malignant hepatoma. Arch Dermatol 1976;112:730.
[Google Scholar]
|
| 7. |
Tajima H, Mitsuoka S, Ohtsuka E, Nakamura Y, Nakayama T, Satoh Y, et al. A case of hepatocellular carcinoma with the sign of Leser-Trelat: A possible role of a cutaneous marker for internal malignancy. Jpn J Med 1991;30:53-6.
[Google Scholar]
|
| 8. |
Thiers BH, Sahn RE, Callen JP. Cutaneous manifestations of internal malignancy. CA Cancer J Clin 2009;59:73-98.
[Google Scholar]
|
| 9. |
Pipkin CA, Lio PA. Cutaneous manifestations of internal malignancies: An over-view. Dermatol Clin 2008;26:1-15.
[Google Scholar]
|
| 10. |
Poole S, Fenske NA. Cutaneous markers of internal malignancy. I. Malignant involvement of the skin and the genodermatoses. J Am Acad Dermatol 1993;28:1-13.
[Google Scholar]
|
Fulltext Views
8,613
PDF downloads
1,582





![[Figure - 1]](#fig_ijdvl_2015_81_3_320_154792_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2015_81_3_320_154792_f2.jpg){kind=link}