Translate this page into:
Malassezia associated hyperkeratosis of the nipple in young females: Report of three cases
2 Department of Dermatovenereology, West China Hospital, Sichuan University, Chengdu, Sichuan, China
3 Department of Microbiology, Meiji Pharmaceutical University, Kiyose, Tokyo, Japan
Correspondence Address:
Yuping Ran
Department of Dermatovenereology, West China Hospital, Sichuan University, 37 Guoxue Road, Chengdu - 610041, Sichuan Province
China
| How to cite this article: Li C, Ran Y, Sugita T, Zhang E, Xie Z, Cao L. Malassezia associated hyperkeratosis of the nipple in young females: Report of three cases. Indian J Dermatol Venereol Leprol 2014;80:78-80 |
Sir,
Hyperkeratosis of the nipple and/or areola (HNA) is an unusual condition characterized by hyperpigmented, verrucous, keratotic thickening of the nipple and/or areola. [1] We report three cases of hyperkeratosis of the nipple associated with Malassezia.
Case 1
A 21-year-old woman had suffered a recurrent papule and effusion on her right nipple [Figure - 1]a for more than 15 years. There was no pain, and the papule was not itchy. The patient had taken advice from a gynecologist and had been followed up for 7 years. However, since no improvement was noted, the gynecologist did a biopsy of the nipple considering breast cancer. Her family history was negative, and the patient had no history of ichthyosis or eczema. A skin examination showed crusting and effusion on the right nipple.
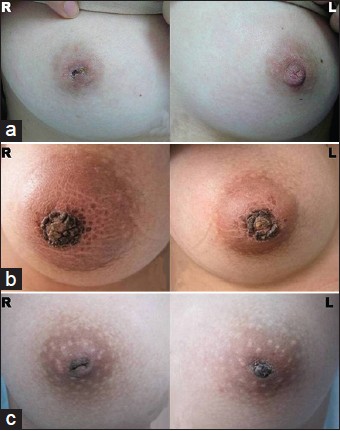 |
| Figure 1: Lesions on the right nipple of patient 1 (a) and on both nipples in patients 2 and 3 (b and c) |
Case 2
A 19-year-old woman with asymptomatic verrucous lesions on both nipples for 3 years was referred to the clinic. The lesions consisted of a round, rough plaque, 2 cm in diameter, on each nipple. They showed dark-brown discoloration and a cobbled hyperkeratotic appearance [Figure - 1]b. The patient was otherwise healthy and had no other skin lesions.
Case 3
A 16-year-old girl presented with a 1-year history of brown patches associated with pain and itching on her nipples. On examination, we found brown, waxy scales on both nipples [Figure - 1]c. The patient′s nipples were inverted. There was no history of eczema, Darier′s disease, or ichthyosis.
Biopsies performed in patients 1 and 3 revealed papillomatous elongation of the epidermis with hyperkeratosis. A number of budding yeast cells were detected in the stratum corneum by periodic acid-Schiff (PAS) and Gomori methenamine silver (GMS) staining [Figure - 2].
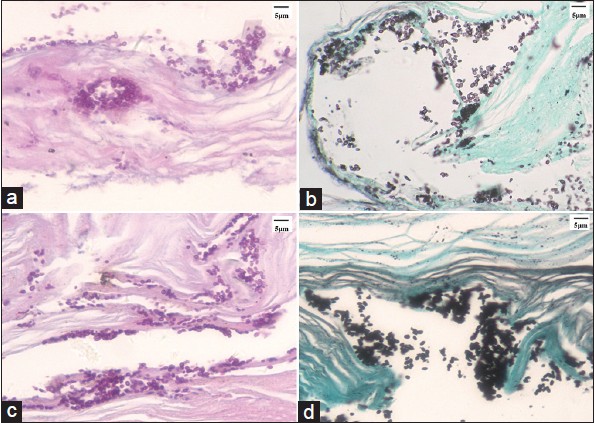 |
| Figure 2: Budding yeast cells were detected in the stratum corneum in cases 1 (a and b, ×400) and 3 (c and d, ×400) by using periodic acid-Schiff (PAS) and Gomori methenamine silver (GMS) staining |
Direct methylene blue staining of scrapings revealed yeast cells in all three patients [Figure - 3]. Scales were cultured and the colonies examined under a microscope, which revealed yeast cells. Three strains recovered from the medium were identified as Malassezia species. Fungal DNA was extracted from paraffin-embedded tissues of patients 1 and 3, and from scales of patient 2, according to the method of Sugita et al. [2] Overall colonization by all Malassezia species and colonization by M. globosa and M. restricta were determined by real-time polymerase chain reaction (PCR) analysis of the samples, performed according to the method of Sugita et al. [2] All samples were analyzed in triplicate. M. globosa was detected in the samples from patients 1, 2, and 3 in all three cases. M. restricta was detected in patient 2.
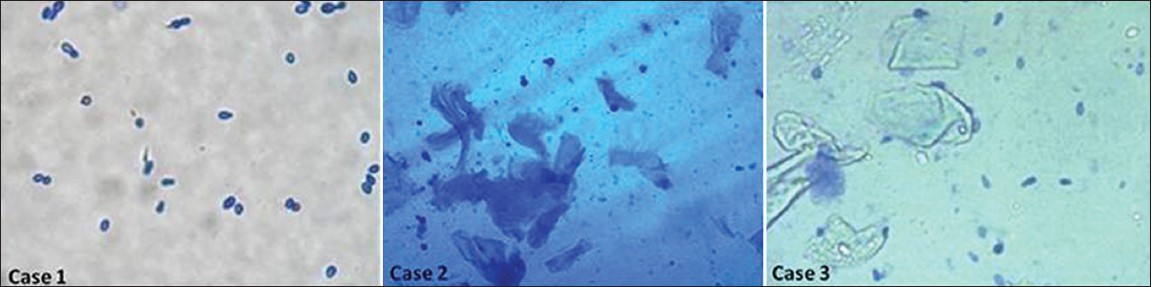 |
| Figure 3: Direct methylene blue staining of scrapings revealed yeast cells in all three patients |
The first patient was treated with oral itraconazole (0.2 g, twice a day) and topical povidone-iodine for 16 days [Figure - 4]a. The other two patients finally improved after treatment with oral itraconazole (0.2 g, twice a day), topical 1% naftifine-0.25% ketoconazole cream, and washing with 2% ketoconazole lotion for 14 days [Figure - 4]b and c, and no yeasts were found by direct mycological examination. No recurrence has been observed in any of the three patients till date.
 |
| Figure 4: All three patients improved after treatment for 14 days |
The three patients were female, in the age group 16-21 years. None of them had pityriasis versicolor or seborrheic dermatitis. Females in this age range often have high levels of estrogen secretion, but endocrinological investigations showed that the levels of female hormones in the three patients were within normal limits. Doppler ultrasonograms of the breasts were normal. We found no evidence that the cases we reported were connected with the endocrine system. While terra firma-forme dermatosis and dermatosis neglecta have similar clinical manifestations, such pigmented plaques could be easily removed using isopropyl alcohol. [3] In contrast, repeated efforts to scrub the affected area with different types of soaps and cleaners, as well as isopropyl alcohol, failed to improve the condition. It is rare that hyperkeratosis of the nipple is associated with Malassezia infection. Malassezia sp. are lipophilic yeasts of the cutaneous microbiota and have been implicated in various diseases, including pityriasis versicolor, seborrheic dermatitis, Malassezia folliculitis, atopic dermatitis, and psoriasis. [4] Taizo et al. reported a case of confluent and reticulate papillomatosis with Malassezia sp. in the lesion. [5] Tamraz et al. reviewed 10 cases of confluent and reticulated papillomatosis, and observed Malassezia yeast in six cases. An improper keratinizing response to Malassezia has been hypothesized as underlying the pathological keratinization. [6] A similar improper keratinizing process may be underlying the three cases reported here. Boralevi et al. reported two cases of hyperkeratotic head and neck Malassezia dermatosis; M. globosa and M. sympodialis were identified from the scrapings. [7] In the three cases reported here, M. globosa were dominant in cases 1 and 3, but M. restricta was detected in case 2. It is still unclear whether the different species are related to body regions or ethnic or geographic background.
In conclusion, Malassezia yeasts were detected in the lesion and antifungal therapy was effective in all these patients; therefore, we consider that Malassezia might be a new factor associated with hyperkeratosis of the nipple. Although it is still unsettled whether Malassezia is the direct cause, antifungal therapy could be considered besides keratolytic therapy, cryotherapy, and retinoid therapy in patients with hyperkeratosis of the nipple.
Acknowledgment
We thank Dr. Xinyu Lin for providing case 3.
| 1. |
Shastry V, Betkerur J, Kushalappa PA. Unilateral nevoid hyperkeratosis of the nipple: A report of two cases. Indian J Dermatol Venereol Leprol 2006;72:303-5.
[Google Scholar]
|
| 2. |
Sugita T, Suto H, Unno T, Tsuboi R, Ogawa H, Shinoda T, et al. Molecular analysis of Malassezia microflora on the skin of atopic dermatitis patients and healthy subjects. J Clin Microbiol 2001;39:3486-90.
[Google Scholar]
|
| 3. |
Lucas JL, Brodell RT, Feldman SR. Dermatosis neglecta: A series of case reports and review of other dirty-appearing dermatoses. Dermatol Online J 2006;12:5.
[Google Scholar]
|
| 4. |
Gupta AK, Batra R, Bluhm R, Boekhout T, Dawson TL Jr. Skin diseases associated with Malassezia species. J Am Acad Dermatol 2004;51:785-98.
[Google Scholar]
|
| 5. |
Hamaguchi T, Nagase M, Higuchi R, Takiuchi I. A case of confluent and reticulated papillomatosis responsive to ketoconazole cream. Nihon Ishinkin Gakkai Zasshi 2002;43:95-8.
[Google Scholar]
|
| 6. |
Tamraz H, Raffoul M, Kurban M, Kibbi AG, Abbas O. Confluent and reticulated papillomatosis: Clinical and histopathological study of 10 cases from Lebanon. J Eur Acad Dermatol Venereol 2013;27:e119-23.
[Google Scholar]
|
| 7. |
Boralevi F, Marco-Bonnet J, Lepreux S, Buzenet C, Couprie B, Taïeb A. Hyperkeratotic head and neck Malassezia dermatosis. Dermatology 2006;212:36-40.
[Google Scholar]
|
Fulltext Views
3,902
PDF downloads
3,124





![[Figure - 1]](#fig_ijdvl_2014_80_1_78_125475_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_1_78_125475_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_1_78_125475_u3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2014_80_1_78_125475_u4.jpg){kind=link}