Translate this page into:
Successful treatment of multiple facial basal cell carcinomas with imiquimod in a patient with chronic renal failure
2 Department of Otorhinolaryngology, Faculty of Medicine, Celal Bayar University, Manisa, Turkey
3 Department of Pathology, Faculty of Medicine, Celal Bayar University, Manisa, Turkey
Correspondence Address:
Aylin T�rel Ermertcan
Department of Dermatology, Celal Bayar University School of Medicine, 45010 Manisa
Turkey
| How to cite this article: Bayata S, Ermertcan AT, Gen�oglan G, Eskiizmir G, Temiz P. Successful treatment of multiple facial basal cell carcinomas with imiquimod in a patient with chronic renal failure. Indian J Dermatol Venereol Leprol 2014;80:195 |
Sir,
We would like to report a case of multiple, pigmented basal cell carcinomas (BCCs) on the face in a patient with chronic renal failure, which responded dramatically to imiquimod therapy.
A 49-year-old woman, with chronic renal failure presented with dark brown patches on her face for 8 years [Figure - 1]a. These were most prominent on her cheeks and had increased in size and number over the years. Dermoscopic examination revealed large, gray-blue ovoid nests, linear and arborizing vessels, maple leaf-like and scar-like areas as well as ulcerations [Figure - 1]b, which were characteristic for BCC. [1] The diagnosis was confirmed by skin biopsy from one of the representative lesions [Figure - 2]. The patient was advised topical application of imiquimod (5%) cream, 5 days a week. This was continued until there was complete resolution on clinical and dermoscopic examination [Figure - 3] in approximately 1 year. Clinical and dermoscopic follow-up of the patient demonstrated no sign of recurrence after 10 months.
 |
| Figure 1 |
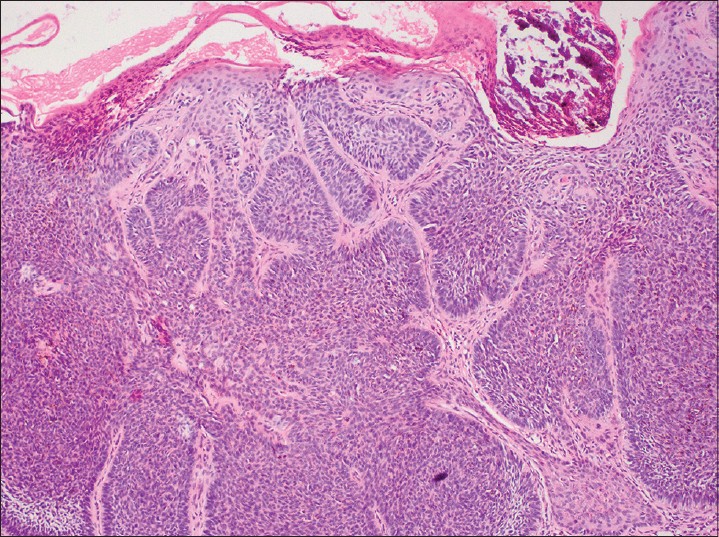 |
| Figure 2: Groups of basaloid cells with peripheral palisading in BCC (H and E, ×100) |
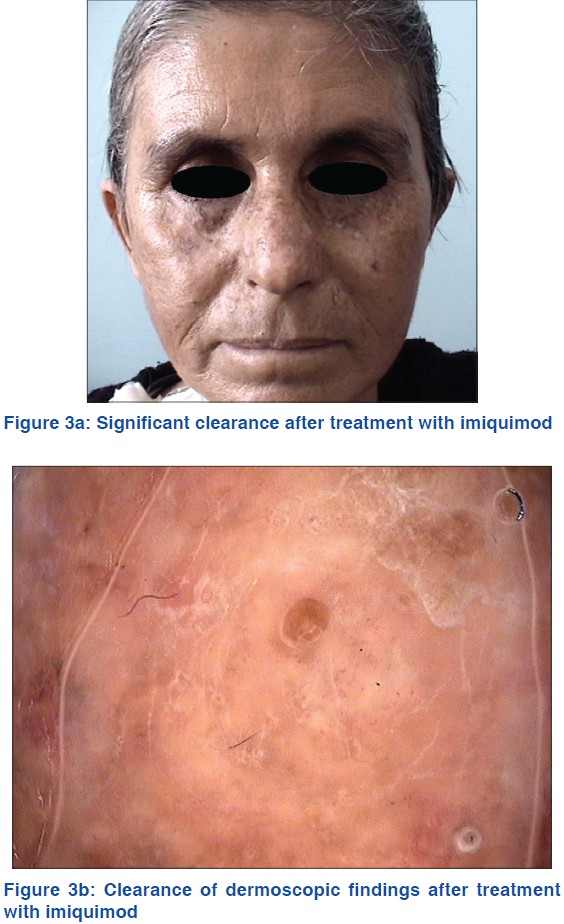 |
| Figure 3 |
BCC is the most common form of skin cancer and accounts for approximately 80% of non-melanoma skin cancers. The major treatment modalities for BCC include electrodesiccation, cryotherapy and curettage, which are often selected for low-risk lesions. However, surgical excision is considered the gold standard because it permits assessment of histopathologic margins. [2] However, excision of multiple facial lesions is generally not preferred due to unsatisfactory cosmetic outcomes. Imiquimod, a toll-like receptor-7 agonist, which belongs to a novel class of immune response modifiers, is a topical agent for the treatment of superficial BCC. It decreases tumor cell proliferation, increases tumor apoptosis and inhibits angiogenesis. It is also a potent inducer of interferon α in vivo, which has potent antitumor and antiviral activity. [2]
Renal transplantation is known to be associated with an increased incidence of non-melanoma skin cancers possibly related to use of immunosuppressant drugs. Both squamous cell carcinoma and BCC, the two major histological types of non-melanoma skin cancers, exhibit a more aggressive biological and clinical course in renal transplant recipients, with higher rates of recurrence and mortality than the general population. [3] The incidence of BCC in the general white population is between 18% and 40% [4] while a study in The Netherlands, revealed that the incidence of BCC in transplant recipients was 10 times higher than the general population. [5]
End stage renal disease is also a cause of immunosuppression in itself as both T and B-cell functions are reported to be altered possibly due to the uremic state. [6],[7] Though there is an increased prevalence of various neoplasms in this setting, [6] specific data on skin neoplasms has not been reported so far.
Our patient had developed multiple and progressive facial lesions of BCC following a diagnosis of chronic renal failure. Her only medications were the anti-hypertensives amlodipine besylate and olmesartan medoxomil. Such multiple lesions may be attributable to the immunosuppression occurring as a part of end stage renal disease . Excision was not considered appropriate for multiple lesions on the face because of the risk of a poor cosmetic outcome Treatment with imiquimod 5% cream led to significant improvement in all lesions.
Imiquimod 5% cream is likely to be a promising agent for the treatment of multiple BCCs in similar settings.
| 1. |
Menzies SW. Dermoscopy of pigmented basal cell carcinoma. Clin Dermatol 2002;20:268-9.
[Google Scholar]
|
| 2. |
Tandon Y, Brodell RT. Local reactions to imiquimod in the treatment of basal cell carcinoma. Dermatol Online J 2012;18:1.
[Google Scholar]
|
| 3. |
Zavos G, Karidis NP, Tsourouflis G, Bokos J, Diles K, Sotirchos G, et al. Nonmelanoma skin cancer after renal transplantation: A single-center experience in 1736 transplantations. Int J Dermatol 2011;50:1496-500.
[Google Scholar]
|
| 4. |
Diepgen TL, Mahler V. The epidemiology of skin cancer. Br J Dermatol 2002;146 Suppl 61:1-6.
[Google Scholar]
|
| 5. |
Hartevelt MM, Bavinck JN, Kootte AM, Vermeer BJ, Vandenbroucke JP. Incidence of skin cancer after renal transplantation in The Netherlands. Transplantation 1990;49:506-9.
[Google Scholar]
|
| 6. |
Laudañski K, Nowak Z. Aberrant function and differentiation of monocytes in end stage renal disease. Arch Immunol Ther Exp (Warsz) 2012;60:453-9.
[Google Scholar]
|
| 7. |
Kim KW, Chung BH, Jeon EJ, Kim BM, Choi BS, Park CW, et al. B cell-associated immune profiles in patients with end-stage renal disease (ESRD). Exp Mol Med 2012;44:465-72.
[Google Scholar]
|
Fulltext Views
2,454
PDF downloads
1,991





![[Figure - 1]](#fig_ijdvl_2014_80_2_195_129439_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_2_195_129439_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_2_195_129439_f3.jpg){kind=link}