Translate this page into:
The safety and efficacy of a combined diode laser and bipolar radiofrequency compared with combined infrared light and bipolar radiofrequency for skin rejuvenation
2 Department of Dermatology, National Medical Center, Korea
3 Chung-Ang University Hospital, Korea
Correspondence Address:
Mi Youn Park
Department of Dermatology, National Medical Center, 245 Euljiro, Jung-gu, Seoul 100-799
Korea
| How to cite this article: Choi YJ, Lee JY, Ahn JY, Kim MN, Park MY. The safety and efficacy of a combined diode laser and bipolar radiofrequency compared with combined infrared light and bipolar radiofrequency for skin rejuvenation. Indian J Dermatol Venereol Leprol 2012;78:146-152 |
Abstract
Background: As the demand for noninvasive procedures for skin rejuvenation is increasing, combined diode laser and radiofrequency and combined infrared and radiofrequency devices have recently emerged. Aim: To compare Polaris WRA TM , a combination device of diode light and RF, and ReFirme ST TM , a combination device of infrared and bipolar RF, in terms of safety and efficacy on skin rejuvenation. Methods: Fourteen Korean volunteers of skin type II-IV, with facial laxity and periorbital rhytids, received three treatments at 3-week intervals with combined diode laser and bipolar radiofrequency (laser fluence 30 J/cm 2 , RF fluence 90 J/cm 3 ) on the right half of their faces and combined infrared light and bipolar radiofrequency (RF fluence 120 J/cm 3 ) on the left half of their faces. Clinical photos of front and bilateral sides of the subjects' faces were taken at baseline and at 6, 9, 12 weeks after the treatment initiation. The investigators' and the subjects' global assessments were performed. Results: There is no statistically significant difference in the overall outcome between Polaris WRA TM and Refirme ST TM based on pre- and post-treatment objective measurements. Polaris WRA TM was more effective than Refirme ST TM at reducing wrinkles when therapeutic results of the two appliances were compared based on the patient satisfaction measurements. After the treatment with both instruments, histological increase in the production and rearrangement of collagen fibers at the dermal layer was observed. The density of the collagen fibers was more increased with the Polaris WRA TM -treated facial area than that of Refirme ST TM . Treatment was generally well tolerated, and there was no serious complication. Conclusion: In this study, both the lasers appeared to be safe, and effective methods for treating skin laxity and facial wrinkles. Combined diode laser and radiofrequency was more effective than combined infrared and radiofrequency at reducing wrinkles and pores when the therapeutic results of both the appliances were compared.Introduction
As desire for beauty increases in the modern society, more patients now focus on maintaining young and healthy skin. The number of patients bothered by facial wrinkles has been steadily increasing, and to resolve this aging problem, they turn the dermatological treatment known as skin rejuvenation. Procedures for skin rejuvenation can be divided into the following two main categories: invasive and noninvasive. In this study, however, only noninvasive method was considered. The standard procedure for this noninvasive treatment is using nonablative laser. It was first developed for skin rejuvenation and skin tightening without damaging the epidermis, and now it is one of the commonly used devices for dermatological purposes. The evolving list of nonablative laser and light systems used for skin rejuvenation includes broadband infrared light (700-2000 nm), pulsed dye (585, 595 nm), Nd: YAG (1064, 1320 nm), diode (910, 1450 nm), and Er: Glass (1540 nm) lasers. [1],[2],[3],[4],[5],[6],[7],[8],[9],[10]
In addition to the nonablative skin rejuvenation, radiofrequency technology is another promising method in the armamentarium. [11] Unlike traditional laser systems that create heat by targeting selective chromophores, radiofrequency technology creates heat by using a tissue impedance, so that the energy becomes a variable dependent on the tissue resistance. [12],[13] However, there has been a study claiming that using only one of the nonablative lasers does not give a full and effective skin rejuvenation. Consequently, Electro-optical synergy (ELOS TM ) technology has been researched to find a way to induce skin tightening and collagen remodeling while reducing the down time. In order to achieve this, a device with ELOS TM technology applies two different types of energy, thus selectively heating the dermal structure while minimizing tissue damage at the same time. [14] Applying these concepts of ELOS TM technology, methods of combining diode laser with bipolar radiofrequency and combining infrared light with bipolar radiofrequency were developed to treat rhytid formation and skin laxity by making changes in deep dermal structure. Although there has been a number of studies that proved the effectiveness of the combination of radiofrequency and diode laser [11],[14],[15],[16],[17],[18],[19] or the combination of radiofrequency and infrared light laser [19] on skin rejuvenation, there has not been a study that compared the efficacy of these two devices.
This study aims to compare Polaris WRA TM , a combination device of diode light and RF, and ReFirme ST TM , a combination device of infrared and bipolar RF, in terms of safety and efficacy on skin rejuvenation by assessing them with both objective and subjective tools.
Methods
Patients
Between July 2008 and December 2008, 14 female patients (mean age: 46 years, skin photo types II-IV) with mild to moderate facial rhytides and cheek laxity were recruited for this study. The exclusion criteria included a history of photosensitivity or recent use of photosensitizing drugs, recent history of any skin disease, operation, systemic disease that could affect skin status, pregnancy, and a history of smoking. Patients were also excluded if they had any other previous aesthetic procedures, such as filler injection, laser resurfacing, chemical peels, or nonablative rejuvenation treatments, within one year prior to the trial.
This study was approved by our institutional review board. Written informed consents for the treatment and for the clinical photography were obtained from all study patients. Three patients who volunteered to undergo biopsies gave their signed consent forms before their entries to the first trial.
Patients received three treatments at a 3-week interval with combined diode laser and bipolar radiofrequency (laser fluence 30 J/cm 2 , RF fluence 90 J/cm 3 ) to the right half of their faces and combined infrared light and bipolar radiofrequency (combined IR 700-2000 nm, 10 W/cm 2 , and RF fluence 120 J/cm 3 ) to the left half of their faces. During each treatment session, patients received three passes over each split faces.
The Polaris WRA TM (Syneron Medical INC., Yokneam, Israel) and ReFirme ST TM (Syneron Medical INC.) were used for treatment in the study. The Polaris WRA TM uses both diode laser at 900 nm and bipolar conducted radiofrequency, and the ReFirme ST TM uses both infrared light at 700-2000 nm and bipolar conducted radiofrequency. While using both lasers, the superficial epidermis was protected from the thermal overload by the contact cooling on the applicator tip. Prior to the treatment initiation, the surface of the skin was hydrated using a thick layer of water-based transparent gel (2-3 mm). Patients were instructed to protect their treated area with a sunscreen with SPF 30 or higher to prevent the occurrence of hyperpigmentation from post-treatment sun exposure.
Clinical assessment
Clinical photos (Olympus E-330) of the front and bilateral sides of the subject′s face were taken at baseline and at 6, 9, 12 weeks from the time of treatment initiation. All assessments were performed by the same physician. The investigator′s and the subject′s global assessments were performed four times; before treatment, 3 weeks after the first, second, and third treatment.
The subject′s assessments and the investigator′s assessments were rated on a five-point scale (worse, no change, fair, good, and excellent). The primary physician and an independent physician rated the wrinkle appearance (compared with the baseline photographs) using the following grading scale-Worse: exacerbation, no change: Improvement of 24% or less, fair: improvement of 25-49%, good: Improvement of 50- 74%, excellent: improvement of 75% or more. Patients were also asked to record any symptoms or signs of adverse effects at the end of each treatment session.
Three patients were selected to participate in the biopsy group. Two couples of 2 mm punch biopsies were performed on their right and left Crow′s feet-the first was taken at baseline, and the second was taken 3 weeks after the final treatment. Specimens were fixed in 10% buffered formalin and routinely processed for Hematoxylin-Eosin (H and E) stain and Masson-Trichrome stain.
Instrumental measurement
A computer-based objective analysis, using Roboskin analyzer (RSA-100; Inforward Co, Tokyo, Japan: which is a state-of-the-art 3D facial imaging system measuring various skin surface conditions by digital photography taken on a fixed platform) was done for all the patients who were enrolled in this study (at baseline and at 6, 9, 12 weeks from the time of treatment initiation). This 3D system measures skin surface structure such as wrinkles, pigmentation, skin tone, and pores, and gives various quantitative and qualitative data through its imaging analysis software.
Statistical analysis
Repeated measures of variance analysis (RM-ANOVA) were used to evaluate the significance of reduction in mean percentage of the wrinkle amount (under eye number, eye side total length, and eye side total area) and the pore open number counts from the baseline to the subsequent assessments. The differences in subject′s global assessments and instrumental measurements were analyzed using paired t-test. Statistical significance was defined as P≤0.05.
Results
Patient characteristics
Fourteen female patients completed the study. The average age was 46 years (ranging between 28 and 58 years) and the Fitzpatrick′s skin phototypes were as follows 7.14% were class II (n = 1), 78.6% were class III (n = 11), and 14.3% were class IV (n = 2). All fourteen patients succeeded to complete the entire study without dropping out.
Clinical efficacy
The Investigators′ Global Assessment is shown in [Table - 1]. The scores indicate the degree of improvement in wrinkle severity, and the scores were higher in the right side of cheek, jowl, and periorbital areas which were treated with Polaris WRA TM . In the nasolabial fold area, the scores were higher in the left side of the face, which was treated with ReFirme ST TM . However, no statistically significant differences between the right and left half of the faces in clinical improvement scores could be observed [Table - 1].

As the study progressed, the statistical analysis showed a significant increase in the investigator′s scores in the right side of cheek, jowl, nasolabial fold areas treated with Polaris WRA TM [Figure - 1] and [Figure - 2], and in the left side of nasolabial fold area treated with ReFirme ST TM [Figure - 3] and [Figure - 4].
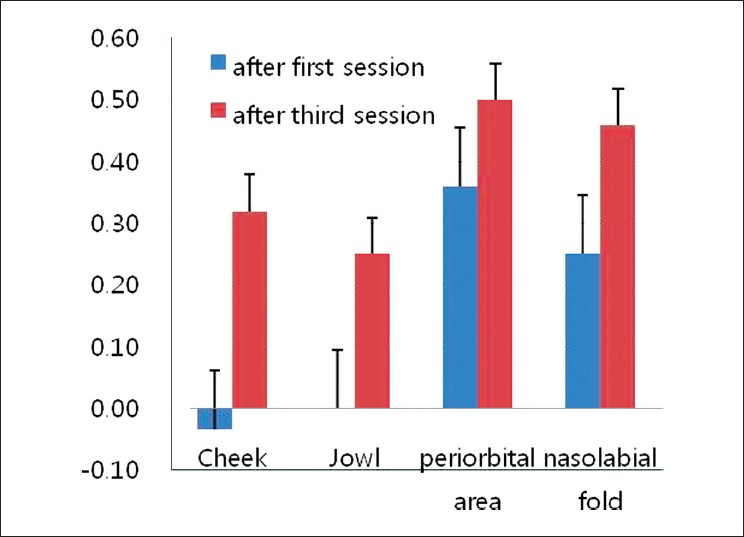 |
| Figure 1: Mean differences of investigator's global assessment of Polaris WRATM (after first session vs third session) |
 |
| Figure 2: Improvement of right periorbital area, cheek, jowl in 42-year-old woman, treated with polaris WRATM (a: Before treatment, b: 12 weeks after the first treatment) |
 |
| Figure 3: Mean differences of investigator's global assessment of ReFirme STTM (after first session vs third session) |
 |
| Figure 4: Improvement of left cheek, jowl, and nasolabial fold area in 42-year-old woman, treated with Refirme STTM (a: Before treatment, b: 12 weeks after the first treatment) |
The Subject′s Global Assessment indicated that there was a positive correlation between the satisfaction of patients and the number of treatment with Polaris WRA TM device (after 12 weeks, 64.3% of the patients expressed that this device had good or excellent effect on their skin). The satisfaction with ReFirme ST TM , however, is rather lower than that with Polaris WRA TM (only 42.8% of the patients expressed good or excellent) results [Figure - 5]. The satisfaction levels of the patients in between each treatment session indicated that in every session, Polaris WRA TM received higher satisfaction than ReFirme ST TM , but there was no statistical significance in this data [Table - 2]. The satisfaction level was higher after three treatments than that after the first treatment in both the devices, but there was no statistical significance [Table - 3].
 |
| Figure 5: The subjects' assessment showed that the overall satisfaction levels with the treatment were higher in right side than left side of face. (a: Subjects' assessment of right side which were treated with polaris WRATM, b: Subjects' assessment of left side which were treated with Refirme STTM) |


Histological analysis
[Figure - 6] is the depicts of H and E stained slides (biopsies on wrinkles near right and left eyes) before the treatment initiation and at 12 weeks after the treatment. It did not indicate any difference in the epidermal layer, but there was a moderate increase in the collagen fibers in dermis, which its difference could not be distinguished between two tested treatments. However, there was a clearer sign of the collagen fiber increase from the right half of the face (Polaris WRA TM device) than from the left half of the face (ReFirme ST TM device) on Masson′s Trichrome stain.
 |
| Figure 6: Significant increase in the amount of collagen was observed by histologic evaluation with standard preparation with H and E (Upper: Before treatment, Lower: After treatment, a: Right side of face, b: Left side of face, H and E, ×200) |
Instrumental measurements
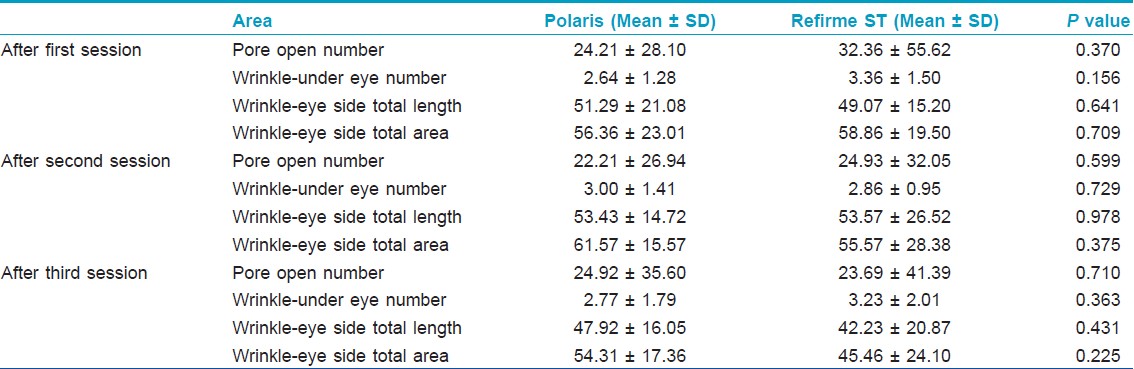
After the first treatment, the skin treated with Polaris WRA TM device showed lower recordings in every area except the Wrinkle -eye side Total length (the score of ReFirme ST TM is 2.214 lower than that of Polaris WRA TM ). After the second treatment, skin treated with ReFirme ST TM device recorded lower measurements in Wrinkle -under eye number (0.143 lower) and Wrinkle -eye side Total area (6.000 lower), while skin treated with Polaris WRA TM device recorded lower measurements in all the other areas. After the third treatment, skin treated with Polaris WRA TM device recorded lower measurement in Wrinkle -under eye number (0.462 lower), while skin treated with ReFirme ST TM device recorded lower measurements in all the other area. However, both devices did not show statistically significant difference in skin improvement when they were compared after each treatments [Table - 4], [Figure - 7].
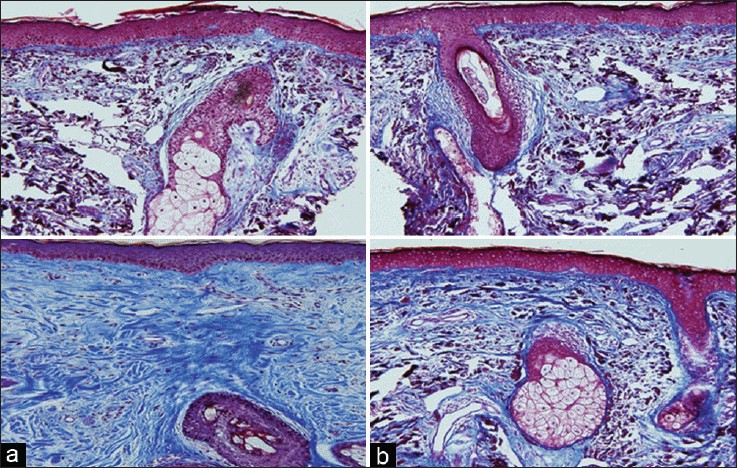 |
| Figure 7: Significant increase in the amount of collagen was observed by histologic evaluation with standard preparation with Masson-Trichrome stain for collagen. Significantly higher collagen density was observed in the right side of face (Upper: Before treatment, Lower: After treatment, a: Right side of face, b: Left side of face, Masson-Trichrome, ×200) |
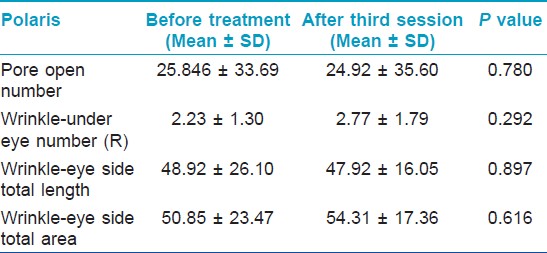
The measured skin condition after the three treatments indicated that the skin treated with Polaris WRA TM device has lesser pore open number and lower Wrinkle -eye side Total length than before the treatments [Table - 5], and the skin treated with ReFirme ST TM device has lower recordings in all the comparable areas [Table - 6]. However, both devices did not show statistically significant improvement of the skin condition.

Discussion
Combined diode laser or infrared light with bipolar radiofrequency were developed in order to treat rhytid formation and skin laxity by changing deep dermal structure. [20] Polaris WRA TM is the device that applies the RF energy and the diode laser simultaneously to treat skin laxity and rhytid. The RF energy penetrates skin and heats deeper tissues to induce neo-collagen production, and the diode laser is used to target more superficial problems, such as pigmentation and visible vascularity. [5] On the other hand, ReFirme ST TM is developed in order to supplement infrared laser, as it may have limitation in penetration depth. When this device is used with RF energy to target water and chromophore inside the skin, it induces skin tightening without pain by applying infrared energy wavelength between 700 and 2000 nm that remodels dermal tissue without damaging epidermis. [19] The speculated mechanism of the diode light energy on dermal structures starts with being absorbed by hemoglobin. After it is absorbed, the diode light energy induces production of the growth factor and cellular mediator (which stimulates wound-healing process), from cutaneous vessel and adnexal structure, indirectly increasing the temperature of the dermis. The infrared light energy, however, is known to be absorbed by water that is included in collagen, and directly produces thermal effect on dermal ground substance. [19] Polaris WRA TM and ReFirme ST TM have two different mechanisms, but yet, there has not been any research performed on comparing these effects on skin rejuvenation. This study could be the first research that compares the effects of Polaris WRA TM and ReFirme ST TM on skin laxity, wrinkle, and structural change on the dermis.
Before conducting this study, the authors of this research experienced that patients′ satisfaction on Polaris WRA TM is rather higher than that of ReFirme ST TM after many years of treatment using both devices. As far as the mechanisms are concerned, it could be speculated that the latter (which induces direct thermal effect on dermis) would result in stronger skin rejuvenation than the former (which induces indirect heating). Yet, the result from the patients showed the opposite from the theory. Based on this difference, this research was started in order to generate objective comparison between two devices.
First, objective assessment based on clinical photographs taken before and after the treatments did not show any statistically significant difference between the two devices. However, as the number of the treatment session increased, statistically significant increase in the satisfaction level could be observed. Patients when rather more satisfied with Polaris WRA TM for the wrinkle improvement, but statistically significant results could not be found.
Although the result of Roboskin analyzer® indicated that there is no statistically significant difference between Polaris WRA TM and ReFirme ST TM for general skin improvements, there were histopathological changes of increasing and rearranging collagen fibers in dermis. In this case, the density of collagen fiber was more increased when treated with Polaris WRA TM than were treated with the other. This result shows a possibility that Polaris WRA TM causes better microscopic skin rejuvenation that its difference from ReFirme ST TM could not be observed through macroscopic observation.
Authors tried to speculate the mechanism that showed how dermis treated with Polaris WRA TM had increased collagen fiber density in all the biopsies. First, ReFirme ST TM is the device that applies broadband infrared spectrum (between 700 and 2000 nm) with optical energy (10 W/cm 2 , which is lower than that of Polaris WRA TM ) to induce clinical improvement of wrinkle and skin laxity. In this way, ReFirme ST TM assures safer treatment with lesser pain than any conventional devices. On the other hand, Polaris WRA TM uses higher optical energy (30 J/cm 2 ) for the initial selective preheating, and emits 570 to 590 nm (targeting superficial vascular lesions) and 900 nm (targeting deeper blood vessel) wavelength laser which might result in more efficient selective thermolysis of the RF energy.
Among all the 14 patients in this research, 12 of them showed signs of pain when their right faces were treated, even though they received local anesthesia using EMLA. Three patients appeared to have erythema, but all disappeared in 2 to 3 days after the treatment. In fact, no erythema was observed in the second treatment.
In this study, objective measurement and the Roboskin Analyzer® were used to objectively compare the effects of the two lasers in improving wrinkles. However, there were few limitations to objectively measure the effects of the two lasers on skin. It was difficult to unify the light intensity for clinical photographs throughout the study, and also, the Roboskin Analyzer® could not recognize subtle wrinkles. It gave different recordings in the same session when the angle between device and skin was distorted even little bit. Besides, we considered that only three patients were selected to participate in the biopsy group is another limitation of this study. However, pathological increase in the collagen fiber density could be clearly observed in both devices. In the authors′ opinions, a larger scale study with more patients might be necessary.
Conclusion
In summary, meaningful difference between two devices was not observed, but there were statistically significant improvements showed in cheek, jowl, and nasolabial fold areas treated with Polaris WRA and nasolabial fold area treated with ReFirme ST at Investigator′s Global Assessment.
Although clinically observable results were present in patients and overall patient satisfaction was low, there was a histological change between before and after the treatments: the collagen fiber in dermis increased and rearranged itself, in which treatment with Polaris WRA showed better result with higher collagen fiber density than that of ReFirme ST.
Therefore, the authors considered that both the devices have improvement in histological aspect and Polaris WRA is a more effective device overall.
| 1. |
Bjerring P, Clement M, Heikendorff L, Egevist H, Kiernan M. Selective non-ablative wrinkle reduction by laser. J Cutan Laser Ther 2000;2:9-15.
[Google Scholar]
|
| 2. |
Rostan EF, Bowes LE, Iyer S, Fitzpatrick RE. A doubleblind, side-by-side comparison study of low fluence long pulse dye laser to coolant treatment for wrinkling of the cheeks. J Cosmet Laser Ther 2001;3:129-36.
[Google Scholar]
|
| 3. |
Tanghetti EA, Sherr EA, Alvarado SL. Multipass treatment of photodamage using the pulse dye laser. Dermatol Surg 2003;29:686-91.
[Google Scholar]
|
| 4. |
Goldberg DJ, Cutler KB. Nonablative treatment of rhytids with intense pulsed light. Lasers Surg Med 2000;26:196-200.
[Google Scholar]
|
| 5. |
Bitter PH Jr. Nonablative photorejuvenation of photodamaged skin using serial, full-face intense pulsed-light treatments. Dermatol Surg 2000;26:835-43.
[Google Scholar]
|
| 6. |
Goldberg DJ, Silapunt S. Histologic evaluation of a Qswitched Nd:YAG laser in the nonablative treatment of wrinkles. Dermatol Surg 2001;21:744-6.
[Google Scholar]
|
| 7. |
Fatemi A, Weiss MA, Weiss RA. Short term histologic effects of nonablative resurfacing: Results with a dynamically cooled millisecond-domain 1320 nm Nd:YAG laser. Dermatol Surg 2002;28:172-6.
[Google Scholar]
|
| 8. |
Muccini JA, O'Donnell FE, Fuller T, Reinisch L. Laser treatment of solar elastosis with epithelial preservation. Lasers Surg Med 1998;23:121-7.
[Google Scholar]
|
| 9. |
Tanzi EL, Williams CM, Alster TS. Treatment of facial rhytides with a nonablative 1450 nm diode laser: A controlled clinical and histologic study. Dermatol Surg 2003;29:124-8.
[Google Scholar]
|
| 10. |
Lupton JR, Williams CM, Alster TS. Nonablative laser skin resurfacing using a 1540 nm erbium glass laser: A clinical and histologic analysis. Dermatol Surg 2002;28:833-5.
[Google Scholar]
|
| 11. |
Kulick MI, Gajjar NA. Analysis of histologic and clinical changes associated with Polaris WR treatment of facial wrinkles. Aesthet Surg J 2007;27:32-46.
[Google Scholar]
|
| 12. |
Ruiz-Esparza J, Gomez JB. The medical face lift: A noninvasive, nonsurgical approach to tissue tightening in facial skin using nonablative radiofrequency. Dermatol Surg 2003;29:325-32.
[Google Scholar]
|
| 13. |
Sadick NS, Makino Y. Selective electro-thermolysis in aesthetic medicine: A review. Lasers Surg Med 2004;34:91-7.
[Google Scholar]
|
| 14. |
Hammes S, Greve B, Raulin C. Electro-optical synergy technology for nonablative skin rejuvenation: A preliminary prospective study. J Eur Acad Dermatol Venereol 2006;20:1070-5.
[Google Scholar]
|
| 15. |
Alexiades-Armenakas M. Rhytides, laxity, and photoaging treated with a combination of radiofrequency, diode laser, and pulsed light and assessed with a comprehensive grading scale. J Drugs Dermatol 2006;5:731-8.
[Google Scholar]
|
| 16. |
Sadick NS, Trelles MA. Nonablative wrinkle treatment of the face and neck using a combined diode laser and radiofrequency technology. Dermatol Surg 2005;31:1695-9.
[Google Scholar]
|
| 17. |
Doshi SN, Alster TS. Combination radiofrequency and diode laser for treatment of facial rhytides and skin laxity. J Cosmet Laser Ther 2005;7:11-5.
[Google Scholar]
|
| 18. |
Kulick M. Evaluation of a combined laser-radio frequency device (Polaris WR) for the nonablative treatment of facial wrinkles. J Cosmet Laser Ther 2005;7:87-92.
[Google Scholar]
|
| 19. |
Yu CS, Yeung CK, Shek SY, Tse RK, Kono T, Chan HH. Combined infrared light and bipolar radiofrequency for skin tightening in Asians. Lasers Surg Med 2007;39:471-5.
[Google Scholar]
|
| 20. |
Sadick N. Bipolar radiofrequency for facial rejuvenation. Facial Plast Surg Clin North Am 2007;15:161-7.
[Google Scholar]
|
Fulltext Views
5,212
PDF downloads
2,518





![[Table - 1]](#tbl_ijdvl_2012_78_2_146_93630_t1.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2012_78_2_146_93630_f7.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_2_146_93630_f8.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_2_146_93630_f9.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2012_78_2_146_93630_f10.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2012_78_2_146_93630_f11.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2012_78_2_146_93630_t2.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2012_78_2_146_93630_t3.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2012_78_2_146_93630_f12.jpg){kind=link}
![[Table - 4]](#tbl_ijdvl_2012_78_2_146_93630_t4.jpg){kind=link}
![[Figure - 7]](#fig_ijdvl_2012_78_2_146_93630_f13.jpg){kind=link}
![[Table - 5]](#tbl_ijdvl_2012_78_2_146_93630_t5.jpg){kind=link}
![[Table - 6]](#tbl_ijdvl_2012_78_2_146_93630_t6.jpg){kind=link}