Translate this page into:
Treatment of nevus spilus with Q switched Nd:YAG laser
Correspondence Address:
Hemanta Kar
Department of Dermatology, STD and Leprosy, PGIMER and Dr. Ram Manohar Lohia Hospital, New Delhi - 110001
India
| How to cite this article: Kar H, Gupta L. Treatment of nevus spilus with Q switched Nd:YAG laser. Indian J Dermatol Venereol Leprol 2013;79:243-245 |
Sir,
Nevus spilus (synonym: Speckled lentiginous nevus) is characterized by dark macules corresponding to junctional or compound nevi over a background of café-au-lait macule (CALM). Speckled lentiginous nevus no longer represents a single entity. Two different variants Nevus spilus maculosis and Nevus spilus papulosis have been described. [1] No standard guidelines exist for its management. [2] Excision, mechanical dermabrasion, ablative and non - ablative lasers have all been tried with varying success. [3]
The present prospective study was undertaken to determine the efficacy of Q switched Nd:YAG laser (QSNYL) in fifteen patients with nevus spilus (NS). Outcome was assessed in relation to reduction of pigment and area of pigmentation using subjective grading score.
Thirty five patients of Indian origin diagnosed as isolated NS were included in the study. Patients were enrolled directly from the Out Patients Department in our hospital as well as from other hospitals in the city during the study period from 2005 - 2011. Skin biopsy was performed in all cases to confirm the diagnosis. Patients underwent multiple treatments performed with 1,064 nm QSNYL (Med-lite C6, USA). Fifteen patients who have completed a minimum of five regular sessions were included. The laser sessions were performed at 4 to 6 weeks regular interval using 1064 nm QSNYL. A combination of 532 nm QSNYL at 3 mm spot size (SS), 2 repetitive rate (RR)and 1064 nm QSNYL, 4 mm SS, 2 RR was used. 1064 nm was used to remove the pigment at dermal level (darker speckles) and 532 nm to remove basilar pigmentation. This combination was used in all the patients. The starting fluence of 532 nm QSNYL was 0.5 J/cm 2 which was gradually increased to 1.5 J/cm 2 at 5 th session (0.5 J, 0.7 J, 1 J, 1.2 J, 1.5 J). 1064 nm QSNYL was used at fluence starting from 3 J/cm 2 to 6 J/cm 2 (3J, 4J, 5J, 6J).
Evaluation of results were made on visual inspection and by comparing serial photographs for reduction of pigment and size of lesion using subjective grading score.
There were 12 females and 3 males, M: F ratio was 0.23. The mean age of the patients was 20.5 years. Minimum age was 14years and maximum age was 35 years. Nine patients (60%) were between 21-30 years of age. Skin type treated included photo type IV in 8 (80 %) patients and photo type V in 7 (20 %) patients. All the patients had nevi since birth. All NS were macular NS. The most common site involved was face in 12 patients. The patients were initially treated with a combination of 532 nm and 1064 nm. The mean number of sessions taken by patients was 8.73.
Of the 15 patients 13 reported some improvement. Two patients reported worsening and developed post inflammatory hyper pigmentation. Four patients reported 25-50% improvement, 6 patients reported 50-75 % improvement and 3 patients had more than 75 % improvement [Table - 1].
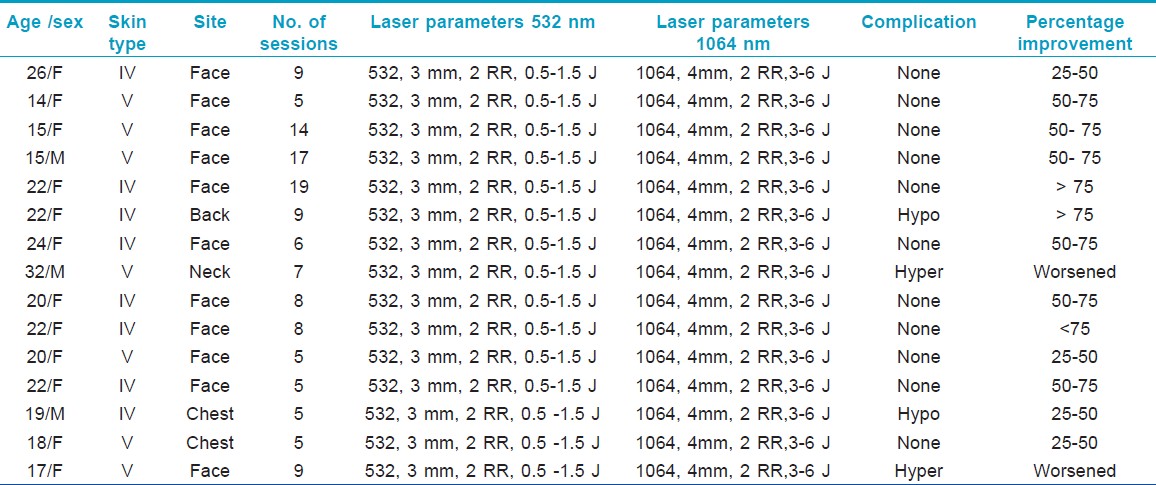
On comparing the number of sessions with percentage improvement, there were 11 patients who received 5-10 sessions and 4 patients received > 10 sessions. Of the 11 patients, 25-50 % improvement was observed in 4 patients, 50-75% improvement was observed in 4 patients and > 75 % improvement in 1 patient. Two patients worsened after treatment. Of the 4 patients who received >10 sessions, 2 patients had 50-75% improvement and 2 patients had > 75 % improvement [Figure - 1], [Figure - 2]. There was statistically significant difference between the number of sessions and the percentage improvement (p< 0.05).
 |
| Figure 1: More than 75% improvement in patient after 9 sessions using Q switched Nd:YAG laser |
 |
| Figure 2: 50- 75% improvement in patient after 14 sessions using Q switched Nd:YAG laser |
Immediate complications were erythema and transient burning after treatment observed in 4 (26.6 %) patients. Mottled confetti like hypo pigmented macules was seen in 2 (13.3 %) patients and post inflammatory hyper pigmentation developed in 2 patients (13.3 %).
Lasers that have been used to treat CALMs and NS are pulsed dye laser, erbium YAG, QS Nd:YAG, Q switched ruby laser (QSRL) and Q switched Alexandrite laser (QSAL). [4],[5],[6],[7],[6]
Q switched systems emitting longer wavelengths (694, 755, 1064 nm) can eliminate deep dermal melanin.
We observed a good clinical improvement in our patients with few side effects. The mean age of presentation was 20.5 years with 12/15 cases involving the face. After treatment improvement was observed in 86.6 % cases (13/15). A direct correlation was observed between the number of sessions and reduction in pigment. Moreover, among the patients who showed improvement, no patient has developed recurrence in the 6 months follow up period. The non responders developed post inflammatory hyperpigmentation within the first 3-4 sessions. All these patients were of type V skin type. They probably need a lower starting dose and gradual increments. Post inflammatory pigmentation was observed in two patients which resolved with depigmentary creams. A cohort study of six patients with Q switched ruby laser showed good results. In a case report which used Q switched Alexandrite laser in a giant nevus spilus also showed more than 50% clearance. [6],[7] However, comparative studies comparing two laser systems and studies on use of Q switched Nd:YAG laser in NS are lacking.
Non-reporting of twenty patients out of 35 enrolled in this study, before the completion of five sessions could be due to financial implications, high expectations with minimal session′s in spite of counseling to every patient before therapy, distance from the laser centre and complications like post inflammatory hyperpigmentation. To conclude, Q switched Nd: YAG laser system can be tried in nevus spilus. However, a larger study with more number of patients and longer follow up is required.
| 1. |
Happle R. Speckled lentiginous naevus: which of the two disorders do you mean? Clin Exp Dermatol 2009;34:133-5.
[Google Scholar]
|
| 2. |
Sigg C, Pelloni F, Schnyder UW. Frequency of congenital nevi, nevi spili, and cafe´-au-lait spots and their relation to nevus count and skin complexion in 939 children. Dermatologica 1990;180:118-23.
[Google Scholar]
|
| 3. |
Polder KD, Landau JM, Vergilis-Kalner IJ, Goldberg LH, Friedman PM, Bruce S. Laser eradication of pigmented lesions: A review. Dermatol Surg 2011;37:572-95.
[Google Scholar]
|
| 4. |
Grevelink JM, González S, Bonoan R, Vibhagool C, Gonzalez E. Treatment of nevus spilus with the Q-switched ruby laser. Dermatol Surg 1997;23:365-9.
[Google Scholar]
|
| 5. |
Tse Y, Levine VJ, McClain SA, Ashinoff R. The removal of cutaneous pigmented lesions with the Q-switched ruby laser and the Q-switched neodymium: Yttrium aluminum garnet laser. A comparative study. J Dermatol Surg Oncol 1994;20:795-800.
[Google Scholar]
|
| 6. |
Moreno Arias GA, Bulla F, Corel VA. Treatment of widespread segmental Nevus Spilus with Q-Switched Alexandrite Laser. Dermatol Surg 2001;27:841-3.
[Google Scholar]
|
| 7. |
Grevelink JM, González S, Bonoan R, Vibhagool C, Gonzalez E. reatment of nevus spilus with the Q-switched ruby laser. Dermatol Surg 1997;23:365-9.
[Google Scholar]
|
Fulltext Views
13,568
PDF downloads
1,642





![[Table - 1]](#tbl_ijdvl_2013_79_2_243_107650_t1.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2013_79_2_243_107650_f2.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_2_243_107650_f3.jpg){kind=link}