Translate this page into:
Trichophyton rubrum onychomycosis in an 8-week-old infant
2 Department of Pathology and Microbiology, Hindu Rao Hospital, Delhi, India
Correspondence Address:
Vinod K Khurana
Department of Dermatology and STI, Hindu Rao Hospital, Delhi 110 007
India
| How to cite this article: Khurana VK, Gupta RK, Pant L, Jain S, Chandra K, Sharma Y. Trichophyton rubrum onychomycosis in an 8-week-old infant. Indian J Dermatol Venereol Leprol 2011;77:625 |
Abstract
An 8-week-old infant presented with 7 weeks history of nail involvement and discoloration. Lesions started over the middle fingernail of right hand at 1 week of age, spreading over to other nails within 2 weeks. Only two nails of the feet were spared. On KOH examination, fungal hyphae were seen and culture showed growth of Trichophyton rubrum. The purpose is to report the earliest case of onychomycosis having multiple nail involvement of fingers and toes (18 nails).Introduction
Onychomycosis caused by dermatophyte infection is rare in infants. The low incidence in infants is attributed to various factors such as rapid linear nail growth rate, a small contact surface area, less chance of trauma, a low incidence of tinea pedis, and an infrequent exposure to fungi in public places. [1] We report a case of 18 nail involvement caused by Trichophyton rubrum in an 8-week-old infant.
Case Report
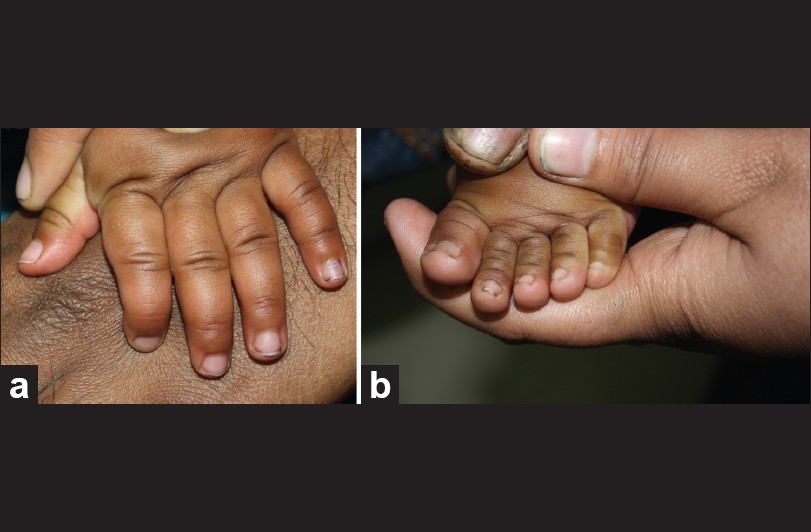
The infant was brought to the dermatology department of our hospital with chief complaints of progressive discoloration, thickening and hardening of fingernails since the age of 1 week. The lesion appeared first on the middle fingernail of right hand. Within 2 weeks other nails were also involved [Figure - 1]a except 2 nd toenail of right foot and 3 rd toenail of left foot [Figure - 1]b.
 |
| Figure 1: (a) All nails of the left hand showing discoloration, thickening and pitting. (b) Toenails of left foot with severe dystrophy and pitting sparing 3rd toenail |
The child was born through full term normal delivery and there was no history of perinatal hypoxia. No congenital malformation was seen.
On examination, distal end of 18 nails showed prominent discoloration, thickening and pitting. Proximal nails showed only pitting and loss of luster. Both the great toenails and left foot 2 nd toenail showed whole nail dystrophy. Clinically 2 nd toenail of right foot and 3 rd toenail of left foot were spared completely. No clinical evidence of tinea manuum or tinea pedis was seen in the infant. Axilla, groin, perianal, and perineal areas also showed no evidence of any fungal infection.
Cutaneous examination revealed no skin lesion suggestive of fungal infection or any other disease. The oral cavity was normal without any evidence of candidiasis. General physical examination and systemic examination were within the normal limits and the developmental milestones corresponded to the age. There was nothing suggestive of any primary immunodeficiency and both the parents were HIV negative. There was no family history of psoriasis, lichen planus, Darier′s disease, pachyonychia linictal, or familial onychodystrophy. There was no history of fungal infection in the family and no contact with any animal source.
On laboratory investigations, KOH preparation showed long hyaline septate-branched fungal hyphae along with conidia, confirming dermatophyte infection [Figure - 2]. Culture showed growth of T. rubrum as white, downy colony with reverse reddish pigmentation [Figure - 3]. Urease test was positive. Fungal culture isolate micrograph also showed large, narrow, cylindrical, long, pencil shaped conidia [Figure - 4]. Histopathological examination of proximal nail was undertaken to rule out common differentials of onychomycosis, such as psoriasis, lichen planus, contact dermatitis and yellow nail syndrome. Only few fungal hyphae which were PAS positive and diastase resistant were found [Figure - 5], on histopathological examination. No other significant finding pertaining to the other differentials were found on histology.
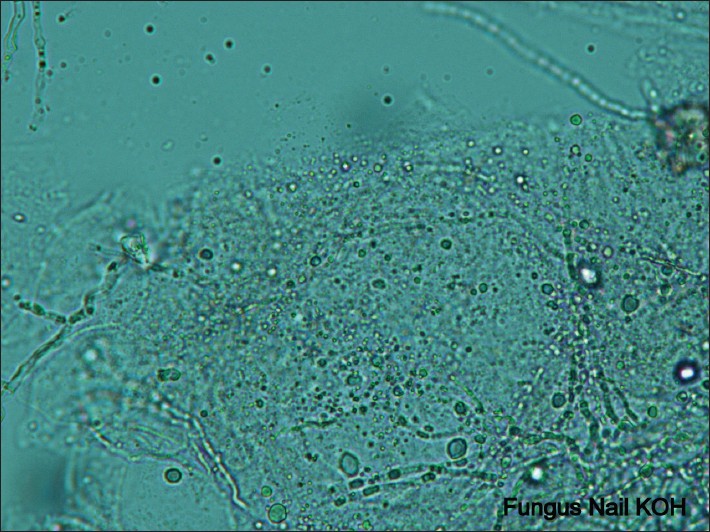 |
| Figure 2: Potassium hydroxide preparation of a nail sample showing branched septate fungal hyphae (Potassium hydroxide, ×40) |
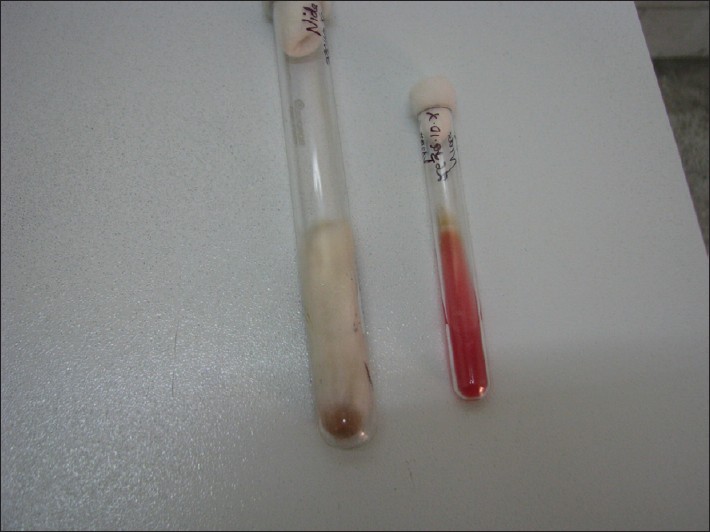 |
| Figure 3: Culture showing white, downy colony with reverse reddish pigmentation |
 |
| Figure 4: Large, narrow, cylindrical, long, pencil shaped macroconidia seen in fungal isolate micrograph (×40) |
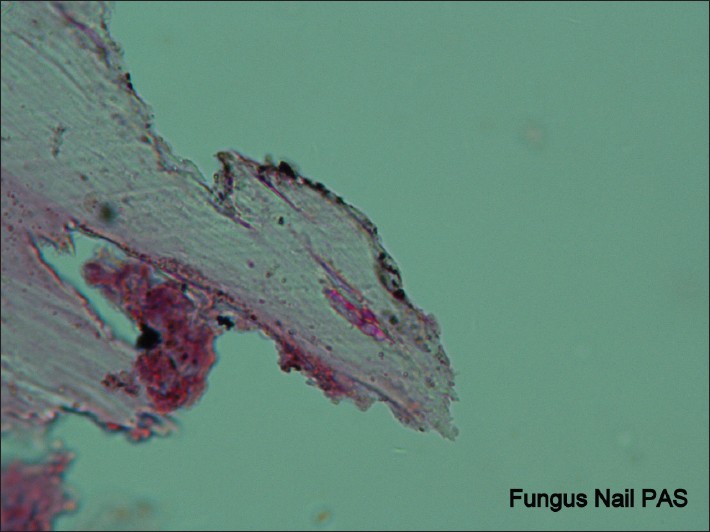 |
| Figure 5: Nail biopsy showing PAS positive fungal hyphae. (PAS, ×100) |
Considering the therapeutic effect and safety profile of terbinafine, the infant weighing 6 kg was given 25 mg/day dose of terbinafine along with 8% ciclopirox nail lacquer for local application. Baseline liver function test and blood count were within normal limits. These parameters were followed up on a monthly interval. After 20 days of treatment, marked improvement was seen in all the 18 nails. There was a decrease in the thickening, pitting and extent of infection in the nail. No side effects of the administered drug were seen. All fingernails were normal after 3 months of treatment with terbinafine without any change in liver function test and counts [Figure - 6]a. All toenails also showed almost complete clinical and mycological cure after 3 months of therapy [Figure - 6]b.
 |
| Figure 6: (a) Clinically cured left hand nails after 3 months of treatment. (b) Cured left foot nails after 3 months of treatment |
Discussion
Onychomycosis is common in adults, uncommon in children and is rare in infants. The most common form of onychomycosis is distal and lateral subungual variant (DLSO) as seen in our case. [2] Distal and lateral subungual onychomycosis is most commonly caused by Trichophyton rubrum.[3] Ahmed and Gupta [4] in their linic-mycological study of onychomycosis also showed Trichophyton rubrum as the most common isolate. In our case both culture as well as KOH examination was positive. The culture of nail clippings from different infected nails showed Trichophyton rubrum. KOH positivity is seen in 80% of DLSO cases and culture is positive in 70% of the cases of onychomycosis. [5] In children less than 2 years of age having onychomycosis, Bonifaz [6] found an association with Down′s syndrome, fungal infection on other body parts, premature birth and perinatal hypoxia, and infection in other family members. These associations were not seen in our infant.
A fungal etiology is unlikely if all fingernails or toenails are dystrophic. [7] However, our case had 18 nails involvement which is very rare. Psoriasis, lichen planus, contact dermatitis, yellow nail syndrome are common differentials of onychomycosis. All differentials were ruled out on histopathological examination of nail biopsy taken from the proximal part of nail.
Generally, systemic therapy is almost always more successful than topical treatment. Topical therapies may be useful adjunct to systemic therapies, but are less effective when used alone. [8] Terbinafine has been used for treatment of childhood onychomycosis. [9] Kobayashi et al. [10] also used terbenafine without any side effects while treating a 9-month-old Japanese girl having kerion. Sardana [11] reported ciclopirox nail lacquer to be safe and effective while treating a 2-week infant with congenital onychomycosis. We also used terbenafine as oral and ciclopirox nail lacquer as topical therapeutic modality in the infected infant.
Onychomycosis is rare in infants. Earliest dermatophyte onychomycosis was reported in an 8-week old infant by Borbujo-Martνnez. [12] Another case was reported by Kurgansky and Sweren [13] in a 10-week-old infant. Both cases reported only few nails involvement. We are reporting a case of 18 nails involvement in an 8-week-old infant. Our case showed complete morphological and mycological cure in 3 months without any side effects.
| 1. |
Baran R, Dawber RP, De Berker DA. The nail in childhood and old age. In: Baran R, Dawber RPR, editors. Nails Diseases and Their Management, 3 rd ed. Oxford: Blackwell Science; 2001. P. 104-28.
[Google Scholar]
|
| 2. |
Hay RJ, Ashbee HR. Mycology. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's Textbook of Dermatology.7 th ed. London: Blackwell Science; 2004. P. 31.37.
th ed. London: Blackwell Science; 2004. P. 31.37. '>[Google Scholar]
|
| 3. |
English MP. Nails and fungi. Br J Dermatol 1976;74:697-701.
[Google Scholar]
|
| 4. |
Ahmad M, Gupta S, Gupte S. A linic-mycological Study of Onychomycosis. Egyptian Dermatol Online J 2010;6:4.
[Google Scholar]
|
| 5. |
Baran R, Hay R, Haneke E, Tosti A. Mycological examination. In: Baran R, Hay R, Haneke E, Tosti editors. Onychomychosis The current approach to Diagnosis and Therapy. 2 nd ed. UK: Informa; 2006. P. 49.
[Google Scholar]
|
| 6. |
Bonifaz A, Saúl A, Mena C. Dermatophyte onychomycosis in children under 2 years of age: Experience of 16 cases. J Eur Acad Dermatol Venereol 2007;21:115-7.
[Google Scholar]
|
| 7. |
Thappa DM. Fungal infections. In: Thappa DM, editor. Clinical Pediatric Dermatology.1 st ed. Philadelphia: Elsevier; 2009. P. 60.
[Google Scholar]
|
| 8. |
Finch JJ, Warshaw EM. Toenail onychomycosis: Current and future treatment option. Dermatol Ther 2007;20:31-46.
[Google Scholar]
|
| 9. |
Baran R, Hay R, Haneke E, Tosti A. Review of antifungal therapy. In: Baran R, Hay R, Haneke E, Tosti editors. Onychomychosis The current approach to Diagnosis and Therapy. 2 nd ed. UK: Informa; 2006. P. 108-9.
[Google Scholar]
|
| 10. |
Kobayashi M, Yamamoto O, Ashai M. Kerion celsi in an infant treated with oral terbinafine. J Dermatol 2001;28:108.
[Google Scholar]
|
| 11. |
Sardana K, Garg VK, Manchanda V, Raipal M. Congenital candidal onychomycoses: Effective cure with ciclopirox olamine 8% nail lacquer. Br J Dermatol 2006;154:573-5.
[Google Scholar]
|
| 12. |
Borbujo-Martínez JM, Fonseca Capdevila E, González Martínez A. Onicomicosis por Trichophyton rubrum en un recién nacido. Actas Dermo-Sifiliogr 1987;78:207-8.
[Google Scholar]
|
| 13. |
Kurgansky D, Sweren R. Onychomycosis in a 10-week-old infant. Arch Dermatol 1990;126:1371.
[Google Scholar]
|
Fulltext Views
6,675
PDF downloads
2,424





![[Figure - 1]](#fig_ijdvl_2011_77_5_625_84069_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_5_625_84069_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_5_625_84069_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2011_77_5_625_84069_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2011_77_5_625_84069_f5.jpg){kind=link}
![[Figure - 6]](#fig_ijdvl_2011_77_5_625_84069_f6.jpg){kind=link}