Translate this page into:
Angiolymphoid hyperplasia with eosinophilia treated with surgical excision and electrocoagulation forceps
Correspondence Address:
Xin-Feng Wu
Department of Dermatologic Surgery, Hospital and Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, Nanjing 210042
China
| How to cite this article: Su YW, Wu XF. Angiolymphoid hyperplasia with eosinophilia treated with surgical excision and electrocoagulation forceps. Indian J Dermatol Venereol Leprol 2016;82:457-458 |
hSir,
Angiolymphoid hyperplasia with eosinophilia is an uncommon idiopathic disorder that presents with plaques or nodules over the skin of the head and neck. They may be isolated or grouped in distribution.[1] Histopathologically, it is characterized by blood vessel proliferation with distinctive large endothelial cells accompanied by a characteristic inflammatory infiltrate that includes eosinophils.[2] Spontaneous remission is known to occur but recurrences are common. Numerous treatment modalities have been reported but results remain unsatisfactory.[3] Treatment is difficult when lesions occur at relatively inaccessible sites such as the external ear canal.
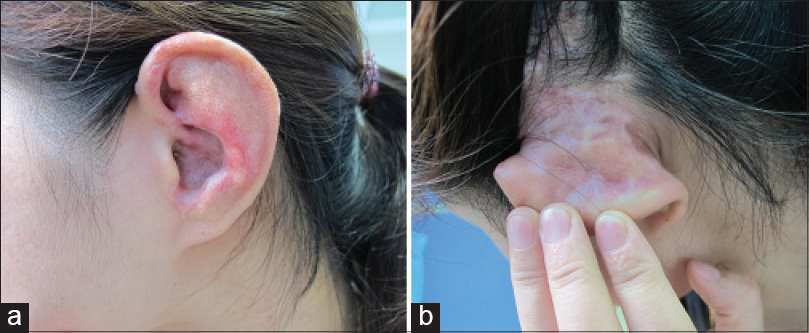
We report a 30-year-old woman who presented with a three-year history of itchy and tender lesions over the left ear, mastoid region and adjacent scalp. These were increasing in size. Cutaneous examination revealed bright red, eruptive papules and nodules ranging in size from 0.5 cm to 1 cm in diameter [Figure - 1]a and [Figure - 1]b. Examination showed no regional lymphadenopathy or any other abnormalities. The routine blood chemistry and urine analysis were within normal limits. The absolute eosinophil count and immunoglobulin E levels were normal. Histopathological examination of a nodule revealed mild epidermal hyperplasia and proliferation of small blood vessels lined by large endothelial cells. There was a dense perivascular infiltrate of lymphocytes and eosinophils [Figure - 2]a and [Figure - 2]b. The clinical and histopathological findings confirmed the diagnosis of angiolymphoid hyperplasia with eosinophilia.
 |
| Figure 1: (a and b) Grouped plaques and nodules involving the skin of the left ear, posterior auricular area and adjacent scalp |
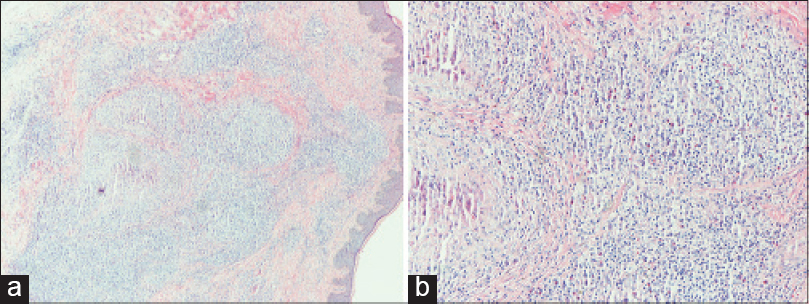 |
| Figure 2: (a and b) Histopathology shows prominent vascular endothelium and perivascular inflammatory infiltration, accompanied by eosinophils. (a: H and E, ×100, b: H and E, ×200) |
We decided to treat the patient with surgical excision and electrocoagulation. Surgical excision was chosen for the scalp lesions because it is considered to be the most effective treatment modality.[2] However, it was difficult to excise the lesions over the ear and mastoid region. Moreover, multiple lesions are difficult to suture. Therefore, we decided to electrocoagulate those lesions using bipolar forceps [Figure - 3]a and [Figure - 3]b.
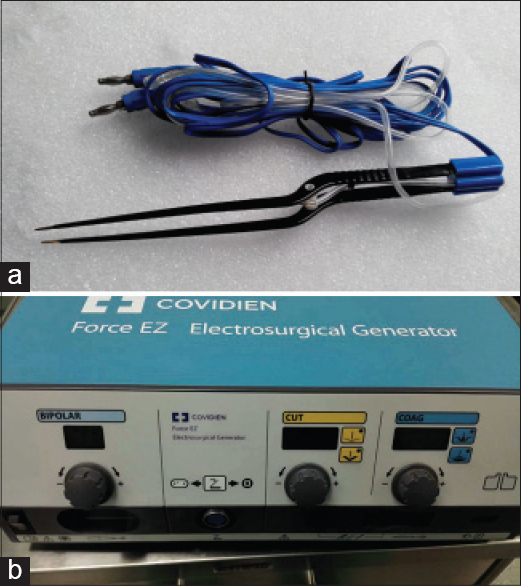 |
| Figure 3: (a) The bipolar coagulation forceps. (b) The electrosurgical generator to which bipolar coagulation forceps was connected |
Half of the lesions over the left ear and mastoid region were electrocoagulated in the first session. The second session was performed two months later to reduce the chances of necrosis in that region. There was some pain over the ear for a few days after treatment. The lesions cleared after two sessions and were no longer pruritic. Some of the lesions healed with depigmentation. There was no recurrence over a follow-up period of nine months [Figure - 4]a and [Figure - 4]b. Overall, the patient was satisfied with the outcome.
 |
| Figure 4: (a and b) Appearance of the lesions at nine months follow-up |
Angiolymphoid hyperplasia with eosinophilia was first reported in 1969 by Wells and Whimster. It is a slowly progressing and self-limiting disease.[1] We should distinguish this disorder from Kimura's disease, angiosarcoma, Kaposi sarcoma and bacillary angiomatosis. Kimura's disease is characterized by vascular proliferation, lymphocytic nodules with subcutaneous germinal foci, fibrosis and edema with deep inflammation. It presents with broad subcutaneous masses, mostly in young adults of Asian descent. In contrast to Kimura's disease, angiolymphoid hyperplasia with eosinophilia may be seen in every race. The lesions are smaller and more superficial. In Kimura's disease, the histopathology shows T-cell lymphoid aggregates with well-formed B-cell germinal foci. However, in angiolymphoid hyperplasia with eosinophilia, there is nodular and diffuse T cell infiltration with small clusters of B-cells. Additionally, Kimura's disease can be differentiated from angiolymphoid hyperplasia by the presence of vascular proliferation and the endothelial cells usually being flat.
Many treatment modalities have been used in angiolymphoid hyperplasia with eosinophilia. Recently, intralesional radiofrequency ablation has been tried in a few cases. There was no recurrence after 4 to 66 months of follow-up.[4] However, electrocoagulation is easier to perform with bipolar coagulation forceps compared to intralesional radiofrequency and other treatment modalities. We were unable to find any previous reports of the use of this novel treatment modality in angiolymphoid hyperplasia with eosinophilia.
Although it may do some harm to adjacent normal tissues, it is safer because the high-frequency electrical energy produced is limited to the region between the two ends of forceps. It can be used at cosmetically important sites with multiple lesions, and is easy to perform. However, it may destroy the shape of the ear to a certain extent. It is important to control the depth of the procedure when using the coagulation forceps and to be careful in areas where important structures such as major nerves and vessels are present underneath.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Wells GC, Whimster IW. Subcutaneous angiolymphoid hyperplasia with eosinophilia. Br J Dermatol 1969;81:1-14.
[Google Scholar]
|
| 2. |
Cheney ML, Googe P, Bhatt S, Hibberd PL. Angiolymphoid hyperplasia with eosinophilia (histiocytoid hemangioma): Evaluation of treatment options. Ann Otol Rhinol Laryngol 1993;102(4 Pt 1):303-8.
[Google Scholar]
|
| 3. |
Chong WS, Thomas A, Goh CL. Kimura's disease and angiolymphoid hyperplasia with eosinophilia: Two disease entities in the same patient: Case report and review of the literature. Int J Dermatol 2006;45:139-45.
[Google Scholar]
|
| 4. |
Singh S, Dayal M, Walia R, Arava S, Sharma R, Gupta S. Intralesional radiofrequency ablation for nodular angiolymphoid hyperplasia on forehead: A minimally invasive approach. Indian J Dermatol Venereol Leprol 2014;80:419-21.
[Google Scholar]
|
Fulltext Views
5,828
PDF downloads
2,510





![[Figure - 1]](#fig_ijdvl_2016_82_4_457_181203_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_4_457_181203_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_4_457_181203_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2016_82_4_457_181203_f4.jpg){kind=link}